
A common refrain in CFS research is that in a sample of CFS patients, 10X of the patients have infection Y and in a control group only X has infection Y. The “Y” may be EBV, Q-Fever, Positive Chronic Lyme tests, or parasites. This is done by researchers trying to identify the cause of CFS using simplistic logic.
To me, the simplest way to KISS these findings is that they are consequences of the CFS state. A reader forwarded me a study “Probiotics for the Control of Parasites: An Overview” [2011] which actually (indirectly) explains why some CFSers have a high incidence of parasites.
Before going into that, let us revisit viral infections (such as EBV, HHV6 etc), many/most are never eliminated, rather your immune system learns to keep them in control. The classic example is the zoster virus which produces chicken pox.
“After you get better from chickenpox, the virus “sleeps” (is dormant) in your nerve roots. In some people, it stays dormant forever. In others, the virus “wakes up” when disease, stress, or aging weakens the immune system. Some medicines may trigger the virus to wake up and cause a shingles rash. It is not clear why this happens. But after the virus becomes active again, it can only cause shingles, not chickenpox.” [WebMd]
We find that “Human populations are infected with 8 herpesviruses, including herpes simplex virus HSV1 and HSV2 (also termed HHV1 and HHV2), varicella zoster virus (VZV or HHV3), EBV (HHV4), cytomegalovirus (HHV5), HHV6, HHV7, and Kaposi sarcoma-associated herpesvirus (termed KSV or HHV8).” [2013] – note that almost all of these have been associated with CFS (i.e. over-represented in CFS patients compared to controls).
We know that CFS patients are low in B12 and that L.Reuteri is the bacteria that produces B12 in healthy people. L. Reuteri is very low in CFS patients . This means they are no protected against these parasites by L.Reuteri which is in abundance with healthy mammals.
Surprise, surprise, surprise! L.Reuteri results in 75+% reduction of many parasites/pathogens including [2011]:
L.Casei also results in similar reduction of:
- Babesia microti
- Giardia lamblia (Giardia intestinalis – [2013])
- Plasmodium chabaudi
- Toxocara canis
- Trypanosoma cruzi
You may being say — what! How can this be! The article does a nice explanation of what probiotics do, namely:
“Modulation of the intestinal environment, by probiotics having the capacity to control the proliferation of surrounding microorganisms and/or by competition for the occupancy of a common biotope (e.g., access to nutriments) [2]. For example, iron is a limiting nutriment: it is essential for most bacteria, and probiotics can compete for its availability. Lactobacillus can render iron unavailable for pathogenic microorganisms, either by binding ferric hydroxide on its surface [4] or by secreting siderophores that chelate and transport iron [3].” So if you are low in Iron, a lactobacillus probiotic may not be ideal.
“Secretion of active molecules (e.g. bacteriocins, antibiotics, free fatty acids, hydrogen peroxide) that can control growth and/or survival of surrounding microorganisms. Bacteriocins are secreted peptides or proteins that generally kill closely related bacteria by permeabilizing their membranes or by interfering with essential enzymes (…. Lactobacillus reuteri produces reuterin (3-hydroxypropionaldehyde), a broad-spectrum antibiotic, active against bacteria, yeast, fungi, protozoa, and viruses [7]. By lowering the local intestinal pH with lactic acid, probiotics can also modify the growth of acid-sensitive organisms [5].”
A second article, “The Unexplored Role of Probiotics on the Parasitic Pathogens. Food and Nutrition Sciences [2014]” reports
“Recent evidences gathered from in vitro culture systems or at best in animal models have demonstrated that probiotic bacteria can be used for therapeutic purposes on control of both intestinal parasite infections as well as few non-gut infections spread among human and veterinary animals. ” and further adds this important finding
“The good effects of probiotics is largely dependent on the dose ingested of at least five billion colony forming units per day for at least 5 days [2009] which acts as a minimum dose for the survival capacity of the ingested probiotics in the gastrointestinal system to overcome the competition with the resident bacteria.” Note: This is 5 billion of a specific species — not grand total of many species!
- “Also, serum of L. casei-treated mice has shown 1.8 (app.) times more nitric oxide concentration which provides a protective effect upon the plasmodial infection. “
Bottom Line
L Reuteri and L. Casei are important probiotics to address parasites. They are also both on my recommend list (being the exceptions to avoiding any random Lactobabillus probiotic — just like Mutaflor(E.Coli Nissle 1917) is the exception for any random E.Coli).
A second take-away is that you want your dosage to be at least 5 billion of a specific species and to take it for 5 days. Any less dosage and it will be a flow thru probiotic that has temporary effect only.
Consider the probiotic below:
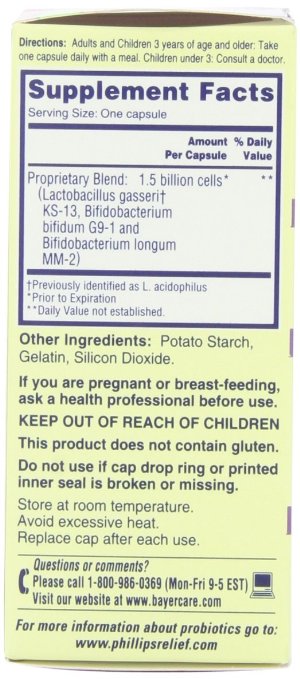
We have just 1.5 billion a day — no way near enough. And there are three species — so an average of 0.5 billion a day of each species… oops… what will NOT happen? (oh,yes — I get it, you will have to keep buying this probiotic!!!) these probiotics will NOT get established.
To quote from an European Probiotic researcher that I have corresponded with “you are outside of the spectrum, because the cfu/g is too low.”
For Miyarisan (Clostridium butyricum) tablets, we read that there is about 10 million viable bacteria per tablet [food.gov.uk] so a full recommended dosage of 18 x 10 million, takes you up to 180 million only.
The research on the needed dosage and duration to establish a probiotic is sparse. There are financial incentive to not release such data (because keeping below that dosage results in constantly repeating customers for the product). The dosage reported above seems “high” but just a few years ago, 400 IU of vitamin D a day seemed very high (and today, 15,000 IU is known to be safe and of great benefit for diabetes, cancer and CFS symptoms).
“While there are no established Upper Limits for probiotic intake, various clinical studies have noted that doses up to 15 billion CFUs of beneficial bacteria have shown efficacy in the maintenance of digestive health/reversing occasional irregularities and doses up to 450 billion CFUs have shown efficacy in the treatment or symptomatic relief of Irritable Bowel Syndrome (IBS).” [Source]
Doing a general search I see that almost every one is keeping below this threshold for any species or have a complex mixture. This site is helpful for finding out tested cfu, https://labdoor.com/rankings/probiotics
- Exception: Culturelle : Single Species 14 Billion CFU [Source]
- Yakult: Single Species 8 Billion asserted
Align was tested to be only 160 million CFU [Source] which means 40 capsule a day to get up to 5 billion.
The rest are BLENDS — Lactobaccillus being in significant quantities. My concern is that different probiotics may compete with each other resulting in less effective CFU (or randomness of which one is the winner!). The same two species (B.lactis and L.Acid.) appear to be the “filler” in many of the mixures.
“The recent publication of the PROPATRIA study (Besselink et ale 2008), which reports higher mortality among subjects with acute pancreatitis treated with a combination of 6 strains of live Lactobacillus and Bifidobacterium species has caused some to question the safety of probiotics. “[Source]
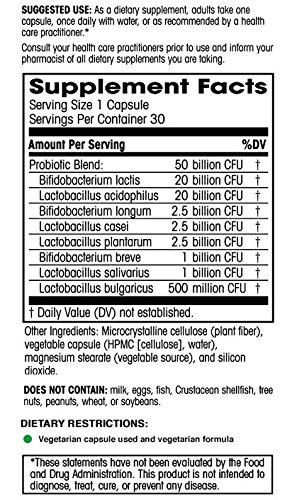
- Healthy Origins® Probiotic 30 Billion CFU’s is a powerful blend of 8 friendly bacteria strains and 30 billion colony forming units (cfu’s) ==> with Bifidobacterium (animalis) lactis and L. acidophilus being above the 5 billion cfu threshold.
- ULTRA-30 Probiotics 30 Billion CFU’s & 18 Strains Supplement ==>
- This one provides two above the desired level, ExtraFlora 50 Billion CFU Probiotics, — one of which is Bifidobacterium (animalis) lactis
“Over the past 30 years there have been about 180 published cases of bacteremia and 69 cases of endocarditis putatively caused by lactobacilli (Aguirre and Collins, 1993; Gasser, 1994; Donohue and Salminen, 1996).” [Source]
