
This page summarizes what is reported on PubMed (excluding Clostridium difficile). Editorial 2015. Update March, 2016 – there are 420+ articles on PubMed
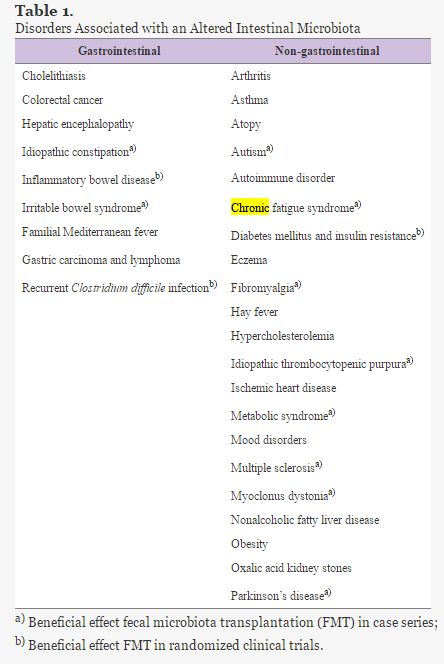
“The high success rate and safety in the short term reported for recurrent Clostridium difficile infection has elevated FMT as an emerging treatment for a wide range of disorders, including Parkinson’s disease, fibromyalgia, chronic fatigue syndrome, myoclonus dystopia, multiple sclerosis, obesity, insulin resistance, metabolic syndrome, and autism” [2016] Table below:
“From a pure technical point of view, FMT is an easy technique that requires a healthy donor (usually a patient’s family member or an anonymous donor), with no risk factors for transmissible diseases or any issues that may alter the cellular composition, particularly prior antibiotic use…. Pinn et al[308] have reported promising results using FMT in IBS patients with refractory disease: 70% of the patients achieving resolution or improvement of the symptoms….randomized, double-blinded, placebo-controlled trials are required.” [2016]
Update
- ” Fecal microbiota transplantation was given on 3 separate occasions from a biological-related donor without success. It was only after a fourth transplant was done with a nonrelated donor that the patient resolved her diarrhea within 48 hours. We suggest that fecal samples from different donors have different abilities to cure Clostridium difficile colitis in at least this immunosuppressed patient.” [2016]
- RBX2660 – A commercial version undergoing trials “Overall efficacy was 87.1% (16 with 1 dose and 11 with 2 doses) for Clostridum difficule. …administration of RBX2660 via enema appears to be safe and effective.” [2016] [2016]- suggests that a single FMT is not ideal.
- “FMT delivered via the lower gastrointestinal seems to be the most effective route for the prevention of recurrence/relapse of CDI.” [2016]
- “the successful utilization of fecal microbiota transplantation to inhibit Klebsiella pneumoniae MBL+ and Escherichia coli ESBL+ gut colonization in the immunocompromised host as a novel tool in the battle against MDR microorganisms.” [2016]
- ” Significant predictors of failure were female sex (P=0.016), previous hospitalization (P=0.006), and surgery before FMT (P=0.005)….” [2016]
- “Based on an analysis of 272 patients, FMT is somewhat less effective in clearing recurrent CDI from patients with IBD, compared with patients without IBD, regardless of immunosuppressive therapy” [2016] hints that CFS/FM/ME without IBS may have better results than CFS/FM/ME with IBS.
Prior
- Improves Quality of Life for IBD and Crohn’s Patient [2015 full text]
- “FMT elicited fever and a temporary increase of C-reactive protein. Abundant bacteria from donors established in recipients, but the efficiency and stability of donor microbiota colonization varied greatly.” [2013]
- “FMT is effective to active UC [ulcerative colitis], the short-term side effects and complications are basically acceptable and controllable. The long-term efficacy and risks of FMT need to be verified further.” [2015]
- “FMT induces remission in a significantly greater percentage of patients with active UC than placebo, with no difference in adverse events. Fecal donor and time of UC appear to affect outcomes.”[2015] 15% chance of remission
- ” At 12 weeks, the microbiota of responders in the FMT group was similar to that of their healthy donors; remission was associated with proportions of Clostridium clusters IV and XIVa.”[2015]
- “This analysis suggests that FMT is a safe, but variably efficacious treatment for IBD.” [2014]
- “The rate of clinical improvement and remission [for refractory Crohn’s disease] based on clinical activity at the first month was 86.7% (26/30) and 76.7% (23/30), respectively, which was higher than other assessment points within 15-month follow-up.” [2015]
- 24% success rate with ulcerative colitis [2015]
- Success for a Crohn’s Patient[2014] [2014][2013]
“US Food and Drug Administration Regulations
In September 2013, the US Food and Drug Administration (FDA) announced that fecal microbiota met the agency’s definition of a drug/biologic substance and that, thereafter, an investigational drug application (IND) would be required to perform FMT for any indication. This decision to apply IND requirements made FMT largely unavailable to the community physician. Permission to perform FMT for the treatment of CDI was granted in emergency cases after discussion with the FDA; however, submission of an IND was still required within 2 weeks of the procedure. In July 2013, after much dialogue and a C difficile fecal transplant public forum, the FDA decided to liberalize the restriction on FMT while maintaining discretionary regulation.
Currently, FDA regulations permit a treating physician to perform FMT for CDI in patients who are unresponsive to standard therapy, without an IND, provided that the physician obtains adequate informed consent. At a minimum, such consent should include a statement that the use of FMT for the treatment of CDI is investigational and a discussion of the potential risks of FMT. The FMT product must be obtained from a donor known to either the patient or the treating licensed healthcare provider. Finally, the donor and the donor’s stool must be qualified by screening and testing performed under the direction of the licensed healthcare provider. The FDA still requires an IND for the use of FMT to treat all other GI and non-GI diseases.” [2014 ]
Comments
Reader: “What are your thoughts on why some of the faecal transplant recipients relapse? Is it possible that the next infection/virus they get triggers the whole process again? Or do dietary and lifestyle factors leave recreate a microbiome over months that becomes susceptible again to a dormant virus that reactivates?”
Relapse: It is impossible to 100% purge a body of bacteria — mouth and nasal bacteria will repopulate the gut. Antibiotics to “clean the body” are not 100%, often just 60% effective.
Consider MRSA — Staphylococcus aureus has kept popping up (causes soluble fibrin monomer, vaccine against produces short term remission) and is very resistant to almost all antibiotics. There are also sleepers which may remain inside biofilms in the gut.
The healthy fecal transplant may not be able to control these “thugs” when they wake up and re-establish themselves.
I believe (no studies) that aggressive rotating probiotic treatment after the transplant for at least 6 months is needed to address these sleepers. By aggressive, I mean higher than recommended dosages.
My recommended recipe for post transplant for at least 6 months (and even before!) is:
- Bifidobacterium probiotics containing many different bifidobacterium species and NO Lactobacillus. 5+ Billion CFU/day
- E.Coli Probiotics (both are made in Germany):
- Symbioflor-2 (6 species) – appears best because one of the species appear to take up residency – can buy on Amazon.de ( 30 drops/ day for 43 days was used in a study to reduce IBS symptoms)
- Mutaflor (1 Species, E.Coli Nissle 1917)
- Increase Variety of species (these do not contain any E.Coli, Lactobacillus or bifidobacterium)
These should be regularly rotated (no longer than 3 weeks on any one of them), to prevent “probiotic resistance” (probiotics produces antibiotics — so we are really say antibiotic (produced by probiotics) resistance!)
I view life style and diet as significant factors for the risk of relapse. Eating out regularly at normal commercial restaurants will likely increase the risk — how much? I don’t know.
I am ex-Microsoft, ex-Amazon — both of those high stress jobs lead to relapse. I no longer pick jobs according to “my capabilities”, “others expectations of me” etc. I pick jobs for what is best for my health. My current job is usually 40 hrs/week (literally!!!) with no company laptop — so when I leave work, I am 100% off the job!!!
