There has been a flood of suggestions over the last year for COVID-19. In general, the suggestions are believers in some cure-all supplements, preaching their gospels. The more responsible one register trials and start (example).
The following are what has studies supporting some speculations.
” the estimated risk of developing respiratory failure was eight-fold lower in patients also receiving oral bacteriotherapy… (Sivomixx® a multi-strain product containing five strains of lactobacilli, two strains of bifidobacteria, and one strain of Streptococcus thermophilus) “
“The formulation administered in this study contained: Streptococcus thermophilus DSM 32345, L.acidophilus DSM 32241, L. helveticus DSM 32242, L. paracasei DSM 32243, L. plantarum DSM 32244, L. brevis DSM 27961, B. lactis DSM 32246, B. lactis DSM 32247. Ormendes SA, Lausanne, Switzerland which gifted the product Sivomixx® (SivoBiome® in USA)”
“a significant predictive power of the four variables: (a) low (<50 nmol/L) 25(OH) vitamin D levels, (b) current cigarette smoking, (c) elevated D-dimer levels (d) and the presence of comorbid diseases”
“Little evidence from observational studies and trials to date have evaluated the effect of high-dose cholecalciferol[Vitamin D] in hospitalized COVID-19 patients.” i.e.
“Results from this retrospective analysis demonstrate that two consecutive doses of 200,000 IU cholecalciferol (total of 400,000 IU) can significantly improve the outcome in patients affected by COVID-19 that are also burdened with three or more comorbid diseases. “
“SARS-CoV-2 patients with acute respiratory distress syndrome show elevated fibrinogen activity, high D-dimer levels and maximum amplitude of clot strength. Platelet count, fibrinogen, and standard coagulation tests do not indicate a disseminated intravascular coagulation. ” [2020]
“the fibrinogen values in patients were higher than the control group (p < 0.05). ” [2021]
Piracetam (where available) may lower fibrinogen levels
A reader asked me about this and I have not had to deal with it but I know it is common. Acid Reflux is also called gastroesophageal reflux disease (GERD). So I am doing a summary of my gold standard sources (a.k.a. PubMed). Internet legends are abundant; I know from prior posts that often they got established from some early study that did not replicate, or was even misread… and the legend just kept going on and on by being repeated. You may also wish to review my 2016 post on this topic
“. After diagnosis, the most common off-label, first-line treatments were:
For US women [2021] “The five factors include normal weight, never smoking, moderate-to-vigorous physical activity for at least 30 minutes daily, restricting coffee, tea and sodas to two cups daily, and a “prudent” diet”
“GERD is common throughout the world, and its epidemiology is linked to the Western lifestyle, obesity, and the demise of Helicobacter pylori.” [2020]
” The represented logistic regression shows that family history of GERD, marital status (divorce), smoking, physical activity frequency, tomatoes/tomato-based foods, salty foods, acidic drinks, frequent use of analgesics, and nonsteroidal anti-inflammatory drugs (NSAIDs) consumption shows statistical significance and association (P < 0.05) with increased risk of symptomatic GERD.” [2020]
GERD takes NSAIDs more than controls
GERD eats chocolate less than controls
GERD eats Tomatoes/Tomato-based food more than controls
GERD drinks more citric drinks than controls
GERD drinks more tea than controls
GERD drinks less pop than controls
GERD smokes more than controls (note: smoking is often associated to stress)
“Sixty-one per cent of students who had a habit of midnight snack for more than three times a week were having GORD symptoms, in comparison to 47% of who did not have the habit.” [2020]
Sixty-one per cent of students who had frequent lack of breakfast for more than three times a week were having GORD symptoms, in comparison to 43% of who did not have the habit”[2020]
Sixty-three per cent of students who had inadequate sleep were having GORD symptoms, in comparison to 45% of who had an adequate sleep.[2020]
” High BMI, family history, energy drinks and fried food were found to be statistically significant risk factors (p<0.05) by univariate analysis.” [2019]
Microbiome changes of the month (which acts as a reserve to bacteria in gastroesophageal) have been seen
“Most gastrointestinal benefits of probiotics have targeted the lower digestive tract, and limited data regarding the upper digestive tract have been reported, particularly for GERD….The aim of this systematic review was to examine the efficacy of probiotics in alleviating the symptoms, incidence, and severity of GERD in the general adult population, as this has not been done before.” [2020]
compared with the placebo, postprandial distress syndrome scores declined significantly with the L. gasseri LG21 intervention (37.5% vs. 17.8%)….the underlying mechanisms of L. gasseri LG21 for improving FD-associated reflux are linked to postprandial effects, involving improved protein indigestion and increased gastric emptying.
Hydrochloric acid (HCL)/betaine/pepsin
This is often suggested on blogging and personal opinion sites. I was unable to find any study supporting it’s use and some studies indicating that with some sub-types, it may make it worst.
“Decreased acid sensitivity in individuals with increasing body mass index may play a pathological role in symptomatic modulation of patients with GERD.” [2019]
“This study shows that a carbohydrate-free diet and/or highly hypoglycidal diet that is enriched with acid pH foods appears to lead to a decrease in the pH of the gastric contents, thus inhibiting the further production of hydrochloric acid with a reduction or disappearance of heartburn symptoms that are typical of gastroesophageal diseases.” [2018] So less HCL results in an improvement.
Herbs / Bitters / Herbal Tonics
While effectiveness is cited in two studies, only a kampo herbal medicine is explicitly named. It may be worth while to try different traditional digestive bitters (as opposed recently created ones)
“The multiple mechanisms of action of medicinal plants[Ceratonia siliqua and rikkunshito] in GERD other than anti-secretory properties appear to provide more efficient treatment and helped to manage the histopathological changes associated with this disorder”
“Although their active components or the mechanism of action were not known by the ancient Persians at that time, their persistent use during different centuries might indicate their effectiveness. Owing to their potential, medicinal herbs are a viable option for the treatment of diseases like GERD even today.”
Bottom Line
As stated above GERD tend to be a western diet disease (and that has been proposed also for the incidence of autism). In terms of life style, the following suggestions should be considered (all of these items appear to be associated to why GERD developed):
Early supper
No evening snacks
Decrease fat and meat content in the diet
No soft drinks, citric drinks or tomato based diet (sorry Pizza lovers!)
Increase chocolate – ideally 70% cacao or more
Daily exercise for 30 minutes
No coffee or tea with caffeine
Work on sleep — melatonin may help with this, and also the microbiome
Lactobacillus gasseri probiotics
REDUCE STRESS in your life — yes, it CAN be done. Stress is a state of mind (move on!).
Thus the whys…
Not having your digestive tract EMPTY by bedtime (think of circadian rhythm for digestive system being off)
Late suppers
Evening snacks
High fat and meat content in the diet (takes longer to digest — see above)
Soft drinks, caffeine(tea, coffee) citric drinks or tomato based diet (sorry Pizza lovers!) – alters bacteria
A lack of exercise (impacts microbiome)
Stress (impacts microbiome)
Sleep issue
Not having a good breakfast (think of circadian rhythm for digestive system being off)
On a bit of a speculative nature, given that the mouth microbiome may be a significant player, altering it may be beneficial. There are three items that I would look at:
Symbioflor® 1 – for illness of the respiratory system, and is likely to also alter the oral microbiome
Two probiotics from Japan that comes as hard tablets suitable for sucking/slowly dissolving in the mouth
I have seen several children (and the literature agrees) with (very) high Bifidobacterium level, typically without an identified species. We not that there are both increases and decreases in Bifidobacteriaceae shown below. PPI should be use with caution.
This BMJ article had a nice graphic of what PPI’s do with red dots indictes higher growth and blue dot with decrease.
I have done a recent review of a child with salicylate sensitivity and in dialog with the parent, I realized that I need to get up to speed on this topic. One of the reasons is that we found that some of the recommendations were matches to some studies for salicylate sensitivity. So far the citizen science analysis at microbiome prescription has not found any specific bacteria associated (not sufficient samples). If you have uploaded a sample AND have salicylate sensitivity, please make sure you have updated you symptoms.
There are many web-sites/blog dealing with salicylates — which given the absence of actual studies, may be worth reading. As always, I will attempt to keep to “gold standard” data sources.
“Major dietary sources of salicylates were alcoholic beverages (22%), herbs and spices (17%), fruits (16%), non-alcoholic beverages including fruit juices (13%), tomato-based sauces (12%) and vegetables (9%).” [2011]
Salicylate poisoning can cause vomiting, tinnitus, confusion, hyperthermia, respiratory alkalosis, metabolic acidosis, and multiple organ failure. Diagnosis is clinical, supplemented by measurement of the anion gap, arterial blood gases, and serum salicylate levels. Treatment is with activated charcoal and alkaline diuresis or hemodialysis.
“Alkalinisation, the mainstay of therapy for salicylate and phenobarbital poisoning over many decades, is effective, although no more so than charcoal, and less than dialysis” [1990]
“Forty-four adults with aspirin poisoning were treated with oral fluids only, standard forced alkaline diuresis, forced diuresis alone, or sodium bicarbonate (alkali) alone. Alkali alone was at least as effective and possibly more effective than forced alkaline diuresis in enhancing salicylate removal. ” [1982]
“One of the more popular and successful treatments has been forced alkaline diuresis to encourage excretion. This technique, however, is not without risk and has now been replaced with alkalinisation alone, which has been shown to be safer and equally successful. The use of activated charcoal as an acute absorbing agent for drug still in the upper gastrointestinal tract is beneficial in minimising further absorption. ” [1992]
“When the urine pH increases to 8 from 5, renal clearance of salicylate increases 10-20 times. Raising the urinary pH level from 6.1 to 8.1 results in a more than 18-fold increase in renal clearance by preventing nonionic tubular back-diffusion, which decreases the half-life of salicylates from 20-24 hours to less than 8 hours. ” [MedScape]
A reader ask me to do a post on the COVID vaccines and people with Chronic Fatigue Syndrome / Myalgic Encephalomyelitis. The risk of death is a significant factor in making a personal decision. This is different than most vaccinations; we need to look afresh at this decision and not run off pro forma decisions for things like measles or extremely low risk-of-infection diseases (polio)
There are possible side-effects, which appear to be transitory for typical people.
A review of unblinded reactogenicity data from the final analysis which consisted of a randomized subset of at least 8,000 participants 18 years and older in the phase 2/3 study demonstrates that the vaccine was well tolerated, with most solicited adverse events resolving shortly after vaccination. The only Grade 3 (severe) solicited adverse events greater than or equal to 2% in frequency after the first or second dose was fatigue at 3.8% and headache at 2.0% following dose 2. Consistent with earlier shared results, older adults tended to report fewer and milder solicited adverse events following vaccination
Aluminum in vaccines: Does it create a safety problem? [2018] “The only problem that deserves attention is the suggested relationship between Al oxyhydroxide-containing vaccines and macrophagic myofaciitis or myalgic encephalomyelitis/chronic fatigue syndrome. Currently, definitive conclusions cannot be drawn on these risks and further studies must be conducted. Until then, Al remains the best solution to improve vaccine efficacy.”
Aluminum adjuvants of vaccines injected into the muscle: Normal fate, pathology and associated disease[2016] Although generally well tolerated on the short term, it has been suspected to occasionally cause delayed neurologic problems in susceptible individuals. In particular, the long-term persistence of aluminic granuloma also termed macrophagic myofasciitis is associated with chronic arthromyalgias and fatigue and cognitive dysfunction.
For people in the US, we have a list of all vaccines and their ingredients here. You will see Human Papillomavirus (HPV) (Gardasil 9) cite above, contains amorphous aluminum hydroxyphosphate sulfate.
The key issue is whether there is aluminum in the vaccine. If there is, it may worsen existing symptoms (especially neurological issues). The bad news is that appears that the current COVID-19 vaccines some contains aluminum (alum) and others do not.
So the traditional and documented issue with vaccines (the aluminum in it) does not apply to two of the Covid vaccines. This implies that for FM, CFS/ME, there is not a supportable evidence-based reason to decline it.
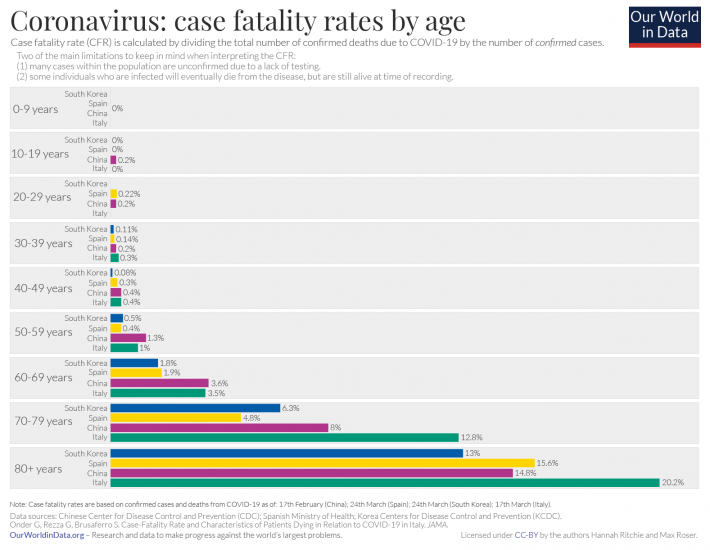
For all ages, the risk of death is significantly higher than for the flu: [see cdc numbers above]
The side effect risks are low and appear to be transient. “Long Covid” – the name given to a CFS-like syndrome after a COVID infection is likely to make any existing ME/CFS or FM much worst. This is estimated that 10% of people are prone. The probable model is that long covid has resulted in a stable gut bacteria dysfunction (for a similar documented-over-several-years similar scenario see this post)
One study of people hospitalized with COVID-19 in Italy found that 87.4% reported experiencing at least one symptom, often fatigue or shortness of breath, 2 months after discharge. Among people with milder infections, however, the prevalence of long COVID has been unclear. Data from the COVID Symptom Study app suggest that 1 in 10 people with the illness experience symptoms for 3 weeks or more
Get the vaccine — there is no evidence-based reason not to (especially if there is no aluminum in it). Not taking the vaccine means significant risk of death and likely more severe CFS/ME or FM.
Post Script – I had COVID… Should I get the vaccine?
Answer is a simple yes. Protection with the vaccine is expected to last longer… Think of it as a booster shot!
I was well trained at University to always work from primary sources (hence the joys of learning at least some greek, latin, french, german, danish for history courses). Bloggers are secondary and often tertiary sources – with the risk of reading more into stuff then there may actually be, or spinning the data to gain readers.
On the flip side, some of their advice comes from experience. The unfortunate aspect of experience is that there is no control for placebo effects, or anti-placebo effects, or effects due to other factors with the person.
“Aspirin enhanced histamine release from basophils via increased Syk kinase activation” [2013]
There is no evidence to suggest that sensitization against drugs occurs more frequently among patients with presumed histamine intolerance compared to patients with normal tolerance to histamine. However, preclinical data suggest interactions between some drugs and histamine catabolism. Nevertheless, the clinical relevance of these findings remains unclear as histamine in humans can be catabolized by different pathways[Editor: DAO and HNMT]. There are no drugs for which induction or worsening of histamine intolerance has been established clinically.
PubMed reports nothing for probiotics that have this effect. Nor for bifidobacterium, nor lactobacillus
For Bacillus, we find evidence of histamine release [1975], exactly the wrong response
DAO Response
There are chemicals/vitamins that DAO and Histamine N-methyltransferase (HNMT) ( the key natural histamine removers) need to act upon histamines. These include:
“Vitamin B6 is a collective term for all 3-hydroxy-2-methylpyridines which act as vitamins. Vitamin B6 substances like pyridoxine, pyridoxal, pyridoxamine, and their phosphorylated metabolites are all equally effective. Pyridoxal-5-phosphate and pyridoxamine-5-phosphate fulfill the functions of a coenzyme in the organism [for activation of DAO].” [2014]
The p values suggests that DAO increased significantly more than histamine.
This may be the source of QAnon belief that citric fruits/vitamin C is bad.
“A cross-over study in former East-Germany on patients who had infection-related asthma found that 5 g/day vitamin C decreased the proportion of participants who had bronchial hypersensitivity to histamine by 52 percentage points (95% CI: 25 to 71).” [2013]
“copper …. did significantly increase two enzyme activities (SOD and DAO)” [1997]
“diamine oxidase (DAO) activity were both increased (linear, p = 0.0004, 0.001, respectively) with Defatted Rice Bran…” [2019]
Negative Impacts
Caution: DAO production seems to increase with gut permeability issues (GPI). Thus something that improves GPI may not actually decrease DAO production, the change of DAO may be a side effect.
“selenium-enriched yeast …significantly decreased the serum concentrations of diamine oxidase (DAO)” [2020] – unclear if the yeast or the selenium was the primary cause.
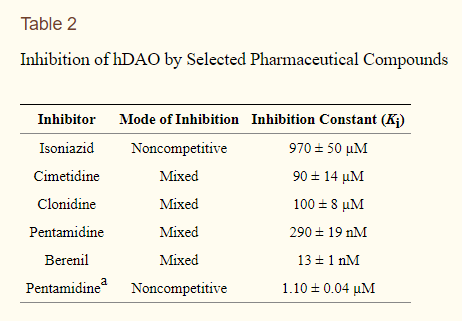
” Antimalarial drugs that inhibit histamine N-methyltransferase also inhibit putrescine catabolism in vivo and DAO activity in vitro” [1981]
“putrescine supplement…. increase in putrescine at 1 h and in diamine oxidase (EC 1.4.3.6) activity within 3-6 h” [1986]
“putrescine is found in virtually all foods of plant origin, and is particularly abundant in fruits and vegetables, notably citrus fruits (1,554 nmol/g) and green peppers (794 nmol/g) (9, 61). There are also high amounts of putrescine in wheat germ (705 nmol/g) and soybean sprouts (507 nmol/g) (37, 70).” [2019]
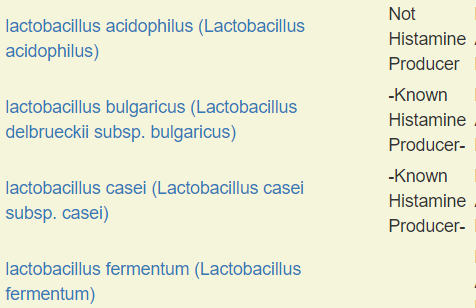
Many probiotics produce histamines, for a list see our commercial probiotic list. For many probiotics, we could not find PubMed studies. Lactobacillus buchneri has been implicated in histamine-poisoning[1991].
See this post to see why strain is often not sufficient, L.Reuteri may or may not produce histamine depending on specific strain.
Foods
Fermented foods are usually uncertain for which bacteria are fermenting it. As we see above, many produce histamine. Studies of commercial Kefir have found that the listed bacteria and the actual are usually in disagreement. Bottom line: no fermented food. This includes sauerkraut, soy, miso, red wine and salami[2020] [1991] .This usually extends into no left-overs, most items left in the fridge (or out) indefinitely– get covered in furry green/black coats. This extends to many cheeses [2020][1995], with Feta Cheese being a possible exception [2020]. For cheese, the same cheese name (like Stilton and Camembert cited below), from one producer may be fine and from another bad — the difference is which strains (not species) of bacteria was used. This also applies to yogurts. For “wild Culture cheeses” it is Russian Roulette for histamines.
Very fresh fish can be safe, but they are prone to producing histamine quickly once skinned [2020].
This also applies to items like nuts and beans that are not fresh.
“Citrus fruits are high in histamines” [Internet Legend?] – alas, I could not find any usable studies. I did find this
In this study, aqueous extracts of peels of best known citrus fruits namely grapefruit (Citrus paradisi), lemon (C. limon), lime (C. aurantifolia) and orange (C. sinensis) were used. Depending on polyphenols content, the extracts were graded as orange > lemon > lime > grapefruit. Effects of the extracts on the release of histamine from rat peritoneal exudate cells (PECs) was measured to know anti-allergic activity. All extracts inhibited the release of histamine from rat PECs induced by the calcium ionophore A23187
“Nasal spray from lemon and quince (LQNS) is used to treat hay fever symptoms and has been shown to inhibit histamine release from mast cells ” [2016]
Other Histamine Producing Foods
In researching another possible internet myth, pineapples and banana. I found a summary of a study which could easily be misread to imply histamine issues. After some effort, I found the full text of the article and shows the results of their lab tests below. The summary stated “Histamine, tyramine, noradrenaline, serotonin and other pressor amines occur in fruits and fermented foods such as bananas, pineapples, cheese and wine. ” It does not state that each is found in every fruit and fermented food
As mentioned above, we should not ignore the amount, fortunately the database behind Microbiome Prescription, allows us to compute across all natural mast cell stabilizers and get concrete numbers.
By amount of Mast Cell Stabilizers
Food
mg/gram
Spices, parsley, dried
4523.25
Spices, celery seed
841.05
Capers, canned
303.89
Spices, saffron
205.48
Dill weed, fresh
68.48
Thyme, fresh
47.75
Elderberries, raw
27.35
Kumquats, raw
21.87
Peppermint, fresh
18.05
Cranberries, raw
16.15
Cranberries, dried, sweetened
12.83
Blueberries, cultivated (highbush), raw
9.53
Blueberries, frozen, unsweetened
7.55
Cranberry sauce, whole, canned, OCEAN SPRAY
6.51
Pitanga, (surinam-cherry), raw
6.2
Acerola, (west indian cherry), raw
5.79
Figs, raw
5.47
Currants, european black, raw
5.16
Raisins, golden seedless
5.11
Prickly pears, raw
5.04
Apples, raw, with skin
4.27
Apples, Red Delicious, raw. with skin
3.87
Blackberries, raw
3.85
Apples, Gala, raw, with skin
3.8
Apples, Golden Delicious, raw, with skin
3.69
Spices, marjoram, dried
3.5
Lemons, raw, without peel
3.07
Olives, ripe, canned (small-extra large) – May be high in histamine [2000]
2.8
Rosemary, fresh
2.55
Apples, Granny Smith, raw, with skin
2.54
Cherries, sweet, raw
2.53
Mulberries, raw
2.47
Cranberry sauce, canned, sweetened
2.44
Apples, Fuji, raw, with skin
2.36
Apricots, raw
2.26
Gooseberries, raw
2.11
Applesauce, canned, unsweetened, without added ascorbic acid (includes USDA commodity)
2
Juice, lemon, canned or bottled
1.83
Plums, dried (prunes), uncooked
1.82
Kiwifruit, green, raw
1.81
Cherries, sour, red, raw
1.71
Strawberries, raw
1.61
Raspberries, raw
1.48
Jujube, raw
1.26
Raspberries, frozen, red, unsweetened
1.14
Juice, pomegranate, bottled
1.11
Apples, raw, without skin
1.07
Strawberries, frozen, unsweetened
0.98
Grapefruit, raw, pink and red, all areas
0.94
Dates, deglet noor
0.93
Sauce, pasta, spaghetti/marinara, ready-to-serve
0.92
Watermelon, raw
0.91
Oranges, raw, navels
0.91
Plums, raw
0.9
Peaches, raw
0.88
Pears, raw
0.84
Oranges, raw, all commercial varieties
0.77
Juice, grape, canned or bottled, unsweetened, without added ascorbic acid
0.75
Melons, cantaloupe, raw
0.72
Nectarines, raw
0.69
Juice, apple, canned or bottled, unsweetened, without added ascorbic acid
0.58
Olives, pickled, canned or bottled, green May be high in histamine [2000]
0.56
Juice, lime, raw
0.51
By Number of different Mast Cell Stablizers
Different flavonoids may have different responses, hence the most varied should also be considered.
Food
Flavonoids Counts
Raspberries, raw
6
Strawberries, frozen, unsweetened
3
Oranges, raw, all commercial varieties
3
Apples, raw, with skin
3
Blueberries, cultivated (highbush), raw
3
Blueberries, frozen, unsweetened
3
Cranberries, raw
3
Kiwifruit, green, raw
3
Lemons, raw, without peel
3
Mangos, raw
2
Melons, cantaloupe, raw
2
Oil, olive, salad or cooking
2
Cranberry sauce, canned, sweetened
2
Currants, european black, raw
2
Dill weed, fresh
2
Elderberries, raw
2
Gooseberries, raw
2
Grapefruit, raw, pink and red, all areas
2
Capers, canned
2
Cherries, sour, red, frozen, unsweetened
2
Cherries, sour, red, raw
2
Cherries, sweet, raw
2
Cranberries, dried, sweetened
2
Apricots, raw
2
Bananas, raw
2
Blackberries, raw
2
Oranges, raw, navels
2
Peaches, raw
2
Peppermint, fresh
2
Pitanga, (surinam-cherry), raw
2
Prickly pears, raw
2
Raisins, golden seedless (because of age, histamine risk)
2
Raspberries, frozen, red, unsweetened
2
Strawberries, raw
2
Thyme, fresh
2
Watermelon, raw
2
Rosemary, fresh
2
Spices, celery seed
2
Spices, parsley, dried
2
Acerola, (west indian cherry), raw
2
Bottom Line
I will gladly take comments citing gold standard sources (PubMed with full test), please do not add comments about so-and-so saying something is bad. I dislike QAnon medicine.
The above should give a framework for diet and cooking, as points
Use items high in mast cell stabilizers
No fermented foods or left overs
No ‘old raw’ ingredients (i.e. nuts, beans, etc) – unfortunately, most of these do not have “Picked dates” on them. Bad storage (i.e. high humidity, temperature) is also a factor.
Dried fruit/vegetables have significant histamine risk
Canned food is unclear, but there are cases of problems from some manufacturers[2010].
Fresh frozen is usually fine. We buy blueberries originating at a far 4 miles away. We know that the temperature is cool when they are harvested and thus the risk of bacterial growth on them is low. Likely much lower than “fresh blueberries” at the market that was shipped from Chile and have been on display for 3 days.
Find out when fruit, vegetables etc are delivered to your market, you want to shop the next day — avoiding all old looking items
Peel fruits etc, immediately before consumption. Skins evolved to protect the contents from bacteria (i.e. histamine producing) growths
Whenever you hear an avoid (example list)— do your homework on it. Use PubMed exclusively. One of the best items for mast cell stabilization is Kumquats, which is on many avoid lists because it is in the citric family…. another QAnon recommendation.
IBS/Gut permeability appears to be a significant co-factor.
Evidence please! Studies, not the volume of people repeating rumors!