There is a giant sphinx of evidence showing that restricted access to the planet’s microbiome is the fundamental etiogenic factor of ME/CFS, but most scientists refuse to face this veritable monument of information.
Let us see a few things.
There are 63 recognized epidemics of the disease, 31 of which occurred in hospitals, just affecting health professionals. The first, in 1934, hit all 198 nurses and doctors at the Los Angeles County Hospital, but curiously, none of the patients admitted to the institution. Until today, the predilection of the disease for health professionals is an undisputed fact; why is that? …
The fact is, health professionals spend most of their lives in aseptic environments, where access to the natural microbiome is blocked. Mechanical barriers (masks, gloves, caps, sterile clothing, disposable aprons, safety glasses, shoe covers), chemicals (frequent washing of hands with detergents, abusive and continuous use of degerming agents (alcohol, chlorhexidine, iodine, hypochlorite, etc.), and even cultural behaviors block the access to beneficial microorganisms. In 2010, I saw in London the recommendation to avoid kisses on the cheeks and handshakes on hospital premises.
Taking the first epidemic of ME/CFS as a paradigm, in 1934 Pasteur had already demonstrated the bacterial origin of the infections, but penicillin was still not available, and the hospital had many infections; hygiene norms were therefore neurotic. In addition, foods were also strictly sterile, and there was a boom in spam and canned foods, considered safer because they were sterile (the occurrence of botulism in the first canned foods led the industry to intensify food sterilization systems in cans).
DeMeirleir et.al. advocate that the ingestion of metals by people living with dysbiosis triggers or aggravates ME/CFS, and the welds of the first cans contaminated the food they contained with toxic metals.
The other epidemics victimized human groups in relatively isolated or restricted coexistence: convents, military bases, schools, a ship, industries, groups of athletes, having in common few interpersonal contacts, and cafeterias with carefully sterile food, aiming at the prevention of food infections. I believe that cold winters also favor the emergence of disease, by limiting the expansion of the natural microbiome.
Besides, considering the Epidemiology of ME/CFS, summarized in Chapter 15, it solidifies the understanding that the greater symbiosis breakdown leads to this confusing spectrum of diseases.
Adding to this set of evidence is the fact that isolated cases of these diseases began to affect middle-aged upper-middle-class women: more acculturated mothers and grandmothers, with access to better sanitation, and higher hygienic standards; determined to make food safer (meaning sterile) for their children and grandchildren.
I am not refuting here any of the hundreds, perhaps thousands, of research that demonstrates countless pathophysiological mechanisms involved in ME/CFS (although many are refutable); I just focus on the essential condition that leads to the development of the disease: the war imposed by civilization on the microbiome of the blue planet.
I am sure that in the near future a good epidemiologist with access to the internet, and with some software or calculator, will confirm my theory; which supports and has been strengthened by the research I have carried out over fifteen years.
In addition, I envision the moment when artificial intelligence resources and/or a broader meta-analysis will seal this knowledge.
This sphinx will not devour me. Neither will those willing to accept the intuitive knowledge that deciphers it.
Se você pesquisar ME/CFS + o nome de um país desenvolvido, e depois outros, você descobrirá que as nações com alto IDH estão lidando com uma doença bizarra, camaleônica, epidêmica e endêmica, debilitante, sistêmica, gravíssima em muitos casos, e associada a suicídios – uma doença que tem uma história incrível e reveladora, e que se expande nas cidades de quase todo o mundo, em especial no Ocidente.
Embora se diga que ainda é muito pouco, há nesses países iniciativas de numerosas fundações, ONGs, universidades, sistemas de saúde, movimentos sociais, profissionais, de clínicas e laboratórios, associações de pacientes, e programas de empresas, voltados à conscientização e ao combate da doença. Recentemente ME/CFS foi discutida no parlamento alemão, e ontem li que fará parte do currículo médico do Reino Unido. Fantástico. Há 18 anos eu estudo a doença.
Holanda, Bélgica e os países da Escandinávia são também especialmente vitimados por ME/CFS, e similarmente desenvolvem programas de educação médica, conscientização, tratamento e prevenção. Na evoluída e gelada Islândia, onde ocorreram surtos epidêmicos, a doença é de tal prevalência que adquiriu designações locais: neuromiastenia, doença de Akureyri, depois doença da Islândia. Nos Estados Unidos, em 2008, ME/CFS foi considerada pelo CDC como o problema de saúde pública mais preocupante no país. No Canadá a prevalência é tão alta ou maior que a dos USA.
São características comuns aos países com muita ME/CFS, um elevado IDH, abundância de alimentos industrializados (esterilizados); e talvez, invernos muito frios. Na Oceania e no Japão a prevalência parece ser um pouco menor.
Um mapa das epidemias de ME/CFS publicado por Donald Acheson em 1959 já mostrava os países-alvo; esses pouco mudaram, o número de doentes é que explodiu.
Acheson, E.D. (1959), The Clinical Syndrome Variously Called Benign Myalgic Encephalomyelitis, Iceland Disease and Epidemic Neuromyasthenia, American Journal of Medicine, 26 (4): 569–595
Entretanto, nas nações em desenvolvimento a história da ME/CFS é outra. Vamos ver?
Pesquise agora ME/CFS + o nome de um país tropical em desenvolvimento: você não encontra nada, ou quase nada. Nesses países a doença é praticamente desconhecida, porque de fato, o número de acometidos é relativamente bem menor. Mas não só por isso.
Esses números se repetem em toda a América Latina, e na maior parte da Ásia: ME/CFS nessas regiões quase inexiste. Nas nações da África, a prevalência é baixíssima, com duas exceções: a África do Sul (onde há IDH alto e invernos frios), e a Nigéria, cuja alta prevalência de ME/CFS é atribuída a malária endêmica; mas que no meu entender deve-se mais ao uso excessivo ou preventivo de antibióticos em razão de grande número de infecções do ciclo da água.
Vamos considerar o Brasil, um país continental, com 215 milhões de habitantes, grandes metrópoles, 546 mil médicos, medicina pujante, hospitais dentre os melhores do planeta, um gigantesco sistema público e universal de saúde, e 357 escolas médicas, o maior número de escolas de medicina no mundo. Não obstante, pesquisando hoje (24 de junho de 2023) no Google usando o Chrome: ME/CFS + Brasil; encontrei apenas um trabalho de 2010 que menciona CFS, nada mais. Nenhuma publicação nos últimos treze anos que sequer mencione a sigla ME/CFS.
Usando o Bing da Microsoft, encontrei apenas uma breve discussão em um Fórum (Fevereiro de 2021) fora do Brasil Brazil: ME/CFS in Brazil | Phoenix Rising ME/CFS Forums., que informava sobre o desconhecimento da enfermidade no país; e revelava o lançamento do primeiro site no país sobre a doença.
Participo de alguns grupos de médicos; dentre 800 profissionais, apenas seis conheciam a doença; dois deles portadores da condição.
E porque isto ocorre?
Entendo que há quatro motivos:
1) A cultura médica do país ignora a existência de ME/CFS, configurando um exemplo clássico de Claude Bernard: o médico não sabe o que procura, e não valoriza o que encontra;
2) muitos pacientes com ME/CFS são rotulados como portadores de fibromialgia, e outros tantos ficam sem diagnóstico;
3) porque há muito menos doença mesmo; restrita às classes A|B, quase três mulheres para cada homem; e …
4) por preconceito dos profissionais de saúde; decorrente de desconhecimento e do problema sem solução que cada paciente traz ou representa; e que fecha o círculo vicioso. Só para citar um exemplo, meses atrás, um renomado colega cardiologista me confessou entre amigos e outros colegas: “eu odeio quando o paciente diz que tem fibromialgia! ”… E completou: “se eu pudesse evitar, eu nem atenderia. ”
Assim é. Por quinze anos, para identificar e conseguir investigar melhor 70 pacientes com ME/CFS, precisei atender em consultório 201 pacientes cujo principal diagnóstico era fibromialgia; outros 39 foram diagnosticados Lyme, fadiga viral, EBV crônico, psicose, etc. Apenas 20 tiveram o diagnóstico inicial de ME/CFS, formulado por mim.
ME/CFS é doença de países ricos, sim; mas não só deles. E não cometa o erro de achar que é desprezível o número de vítimas da ME/CFS no Brasil e nos demais países em desenvolvimento; nas parcelas mais privilegiadas nesses países milhares vivem sob um IDH elevado; e similarmente desenvolvem a condição e enchem os consultórios mais luxuosos, e as relativamente novas clínicas da dor.
Importante, no início de 2020, muito antes de ser descrita a coexistência de ME/CFS e complicações da Covid hoje conhecidas por Covid Longa, antevi o que hoje são fatos: que a incidência de ME/CFS explodiria no mundo pós-Covid, e que as sequelas ou efeitos tardios do coronavírus se somariam ou confundiriam com ME/CFS – que as pandemias se entrelaçariam.
Os resultados da pesquisa, a vivência com os pacientes, e os dados da literatura impõem reconhecer que o fator etiogênico fundamental à ME/CFS é o distúrbio ambiental hostil que leva à quebra da grande simbiose; entendida a grande simbiose como o relacionamento complexo e vital que precisamos manter com o mundo microbiano, e que rompido impõe gravames à homeostasia e leva ao estado de doença.
São muitos os exemplos da nossa dependência da flora. Os médicos conhecem o problema hemorrágico que decorre de antibióticos. Esses medicamentos reduzem no intestino a população de bactérias que produz a vitamina K, necessária às proteínas da coagulação. Sem essas bactérias, sem essa vitamina, podemos apresentar sangramentos.
A título ilustrativo, em elegante post de Elena Panzeri, o infográfico abaixo revela 35 metabólitos do microbioma que participam do desenvolvimento, da função e da integridade do cérebro humano.
by Elena Panzeri
A lista é outro exemplo dos princípios vitais que são fornecidos pelas microscópicas criaturas que nos cercam e que levamos conosco; cuja escassez, desequilíbrio, ou interação anômala em um ambiente inóspito, leva ao que conhecemos por ME/CFS. Faz sentido supor que o mesmo ocorre para todos os outros órgãos e sistemas.
O paradoxo de uma doença dita incurável, mas que apresenta um índice de 4% a 8% de curas espontâneas reforça essa convicção. Essas curas ocorrem pelo restabelecimento da grande simbiose – casual, deliberado ou profissionalmente orientado.
Hoje li um artigo em que a autora advoga a necessidade de cuidado nas tentativas de restaurar o microbioma nos pacientes de ME/CFS, com o que concordo plenamente; é difícil. Mas não concordo com a doença viral que ela advoga ser a causa da doença.
A causa é a privação e a destruição dos microrganismos benéficos no entorno e na vida dos acometidos. Dito de outra forma, a causa é a vitória da civilização na estúpida guerra imposta aos microrganismos dos quais dependemos para viver e ter saúde. Por medo das infecções, resolvemos que deveríamos destruí-los a todos, maléficos e benéficos, de todas as formas. O resultado é ME/CFS. Só não vê quem não quer.
Já postei repetidamente aqui, que uma vez instalada, ME/CFS é um transatlântico pesado que saiu da sua rota levado por uma corrente forte; corrigir o seu curso é geralmente um processo lento, cansativo, sofrido.
O que chamo de ambiente antibiótico é o ambiente hostil ao microbioma da vida urbana, com elevado padrão de saneamento, higiene excessiva, água clorada e fluoretada, e reduzidos contatos sociais. O ambiente antibiótico está nos hospitais e na vida dos profissionais de saúde; pode ter início no nascimento cirúrgico, asséptico, e se expandir na vida dos solitários, das pequenas famílias, nos apartamentos sem animais e plantas; e nos detergentes e antissépticos em todas as suas formas, no uso excessivo de antibióticos e antifúngicos, de desodorantes e desodorizantes, de álcool-gel, de antissépticos bucais; está no fast-food, e nos alimentos estéreis, principalmente os industrialmente processados; nos aditivos e agroquímicos adicionados; na pasteurização, no UHT, nos alimentos irradiados, nas conservas, nos enlatados.
Há uma quantidade enorme de substâncias químicas e antibacterianos nos alimentos industrializados, sendo lícito crer que danificam a nossa flora.
No alimento humano, esse logotipo simpático, verde, ECO, com cara de natural, de orgânico, é o radura logo. Ele sinaliza que a sua comida foi irradiada.
Radura Logo | Alimento Irradiado
A irradiação é a pasteurização do século 21.
A radiação não fica no produto e teoricamente o alimento irradiado não faz mal; mas o bem que faz é limitado; ela torra o DNA de qualquer forma de vida, mata todos os fungos e bactérias; estende a validade e a duração dos produtos. Laticínios perdem vida (morrem os fermentadores), são plastificados e ganham aromatizantes para ter sabor; e a banana no invólucro plástico dura mais de um mês na prateleira.
É relevante a informação de que ME/CFS não existe no povo simples, nem no ambiente rural no Brasil.
O oposto de ME/CFS é a vida no campo, está nas casas cheias, com comida de verdade, feita por mãos, com ingredientes frescos. Está na água dos rios, na horta e no jardim, nos pés descalços, no sexo desprotegido, na praia, na cerveja artesanal, no vinho, nos animais domésticos, no leite fresco, no alimento fermentado em casa. Tenho exemplos e testemunhos de pessoas que ficaram curadas por mudanças no estilo de vida. A adoção de um estilo probiótico de vida, o que inclui o consumo de variados probióticos naturais, gradualmente produz melhora do quadro clínico.
Há um vídeo do fim da pandemia, em que o famoso ator brasileiro Lima Duarte narra a sua infância em que acordava com o pai nas madrugadas, para levar o bezerro ao pé da vaca e conseguir ordenhá-la. Ele diz que é o amor da vaca pelo bezerro que a faz liberar o leite; e profetiza que outras pandemias virão, porque estamos vivendo errado – que falta o amor da vaca no leite da ordenha mecânica. E o que é mais grave, eu acrescento: falta também o microbioma dela e do bezerro, meu caro.
ME/CFS é a menina dos olhos de quem vende diagnósticos e tratamentos, financia ou realiza pesquisas, cria produtos, informação, e tecnologia para tratar os sintomas de uma doença dita sem fim, que tanto sofrimento produz – e que também é terreno vasto e fértil para todo tipo de charlatanismo.
Para impedir conflito de interesse, todo o trabalho médico da pesquisa foi pro bono. Todos os pacientes foram retornados aos colegas que os encaminharam.
In several moments of medicine, the cure was discovered before the cause of the disease was known. Hippocrates treated the anemia of women and children by giving them blackened water from a vase where he left a sword immersed for a few days: iron oxide and ferrous sulfate, the same active principles of medicines that we still use today to treat sideropenia.
In 1747, through the first clinical trial in history, James Lind discovered that citrus fruits and spruce beer cured scurvy, a terrible disease that killed thousands of English sailors, two centuries before the discovery of vitamin C, whose history is a special chapter in medicine. There are many other examples.
In the last half-century, many new epidemic and endemic diseases of insidious behavior have increased and continue to grow in the world, especially in the most civilized regions of the planet; and the sum of evidence points to the depletion and breakdown of the symbiosis with the microbiome as the main factor associated with these many conditions.
The fact is, as we barely understand how it operates or how we actually interact with the microbiota of the planet; and its composition is so vast, and the interactions so complex that we cannot yet speak of causalities, but only of associations. And there are so many associations, and the spectrum of clinical conditions is so varied, that there is no way to escape the recognition that the breakdown of what I have called the greater symbiosis is indeed the cause of this variety of ills, which are even intertwined.
Thus, science associates the altered microbiome with conditions such as allergies, sensitivity to multiple substances, ulcerative colitis, necrotizing enteritis of newborns, inflammatory bowel disease, rheumatoid arthritis, multiple sclerosis and other autoimmune diseases, diabetes, atopy and asthma, cardiometabolic diseases, and cancer. Plus those strange conditions that I didn’t see in medical school, but are now part of my daily life: epidemic gastroesophageal reflux disease, pandemic h. pylori and gastric disease, non-celiac gluten intolerance, endemic obesity, panic disorder, irritable bowel syndrome, autism, ADHD, anxiety, depression suicide complex. The list is much longer, and growing.
If we consider the history of ME/CFS (myalgic encephalomyelitis/chronic fatigue syndrome/fibromyalgia) we find that those are conditions of people and human groups that, in different ways and always for reasons related to civilization, have distanced themselves from nature, from the symbiosis with the microcosm. And this led to some very strange things, like the Gulf War Syndrome – in which ailments in veterans caused by factors directly related to the war entangle with (a disease identical to) ME/CFS that afflicted them, but also the non-military personnel who were in the war, such as administrative staff and members of the press. And more strangely, many of their family members – people who have never been to the Middle East.
Going back to the first paragraph, the fundamental etiogenic factor for scurvy in sailors was the prolonged time at sea, more specifically the prolonged distance from land, where there was a vital principle that did not exist in the sea: vitamin C.
Seen from this perspective, civilized humans are now experiencing A NEW SCURVY, a set of diseases with a common etiogenic factor: the distancing of the natural microbiome; and this time not from land, but from Earth.
Again, the letter C represents a huge contingent of the affected, because according to the CDC it is in the class C of the United States that ME/CFS expands most in the country. It is in microbiome environments similar to that in which the North American class C lives that the disease expands in the world. The environment with sanitation, hygiene, and sterile food that only people from classes A-B reach in emerging countries. The same environment veterans were in during the Gulf War – and outside of it, their families.
In the environment of the 2001 Gulf War, military vehicles represented the British ships of the 17th and 18th centuries. Nowadays, the fear of water-cycle diseases has given rise to a portentous capacity to produce sterile military rations and drinking water, totally deprived of the microbiome; and which represents the new scurvy, the diet of those English soldiers in their old ships, deprived of a vital principle from which they should never split.
In the recent past, when a few hundred proteins and antibodies made it difficult to understand the HLA System, it took the intervention of a mathematician to unravel the complexity of that system, which today involves thousands of proteins.
However, our relationship with the microbiome is infinitely more complex. And although it has been easy to understand how a single kind of microorganism causes a disease (such as trypanosomiasis), or how two types of pathogens cause a disease (Paul-Vincent’s angina, and long-term salmonellosis); or how a single type of microorganism causes more than one disease (such as VZV causing chickenpox and herpes zoster, or EBV that determines mononucleosis and Burkitt’s lymphoma), understanding our interactions with millions of microorganisms that interact with each other and participate in the integrity and function of all living forms will indeed be an almost impossible, spectacular feat.
However, everything leads us to believe that meta-analyses evaluated by artificial intelligence under quantum computing, will soon be the power capable of showing the homo sapiens the fascinating dance of the micro-world with all living things is really like.
Attached you will find a PowerPoint PDF with a YouTube presentation. The target audience is Medical Practitioners treating ME/CFS and Long Covid.
Parallels between Hans Christian Andersen’s “The Emperor’s New Clothes” and the certainty of correct identification of bacteria often expressed by many microbiome researchers should be noted. “Andersen altered the source tale to direct the focus on courtly [academic] pride and intellectual vanity “
A detailed walk through targeted for Medical Practitioners on using the Microbiome to treat Long COVID and ME/CFS. New findings on strong associations (P less than 0.001) derived from the microbiome to these conditions. Discussion of how these finding can lead to treatment suggestions on an individual basis (instead of generic suggestions). Associations listed in full at:
Microbiome tests are not as precise as marketed. Tests have almost zero agreement with each other.
Using test data with data from Kyoto Encyclopedia of Genes and Genomes produces extremely strong consistent associations to the absence (usually) or surplus of specific compounds across three different types of microbiome tests
Working with this data quickly becomes very complex and require advance operations research techniques.
To date, the results of this complex model has been in agreement with the literature (cross-validation), been show on individuals to objectively improve the microbiome with significant subjective improvement.
A few years ago I wrote A Frugal List of Supplements for ME/CFS using knowledge at that time trying to rank order supplements that may help by best cost. Today a similar question came up. I am retired (72 y.o.) and working part time with a variety of complex conditions in the household so getting the right stuff at reasonable cost is a priority.
In this post I will share what our current strategies are and illustrate cost savings. For making our own capsules, I have ignored the cost (since it is low).
Example #1 Supplement Hesperidin
Choice #1: Off the shelf: 13.57 / ( 0.500 g x 60) = $0.45 per gram
Choice #1: Off the shelf: 30 capsules with 10 BCFU: $12.42 / (30 x 10) = $0.04 / BCFU
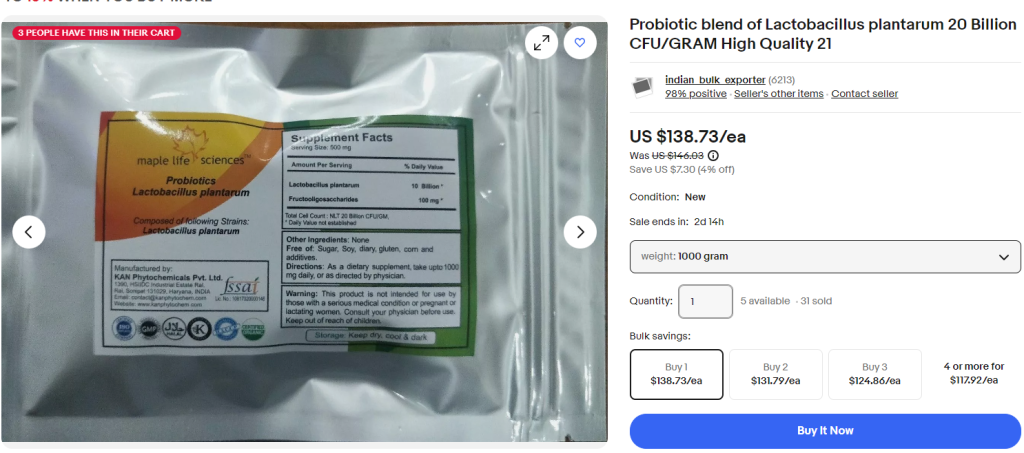
Choice #2: Bulk Probiotics as powder: 169.17 / (400 x 100) = $0.004 per BCFU. Lower package sizes available at slightly higher cost per BCFU.
Choice #3: Buying direct from a manufacturer in bulk (Organic and typically manufactured within 2 weeks of shipping): $138.73 / (20 x 1000) = $0.007/BCFU. Lowest package is $0.02/BCFU
A key issue is probiotics is time since manufacture, abuse in storage (i.e. not kept is fridges in transit and storage — if you look “behind the scenes” at many health food stores, you will see boxes of probiotics just kept in the back, not refrigerated. They are then put it into the display refrigerator as needed). See Probiotics — what is advertised may not be what you get
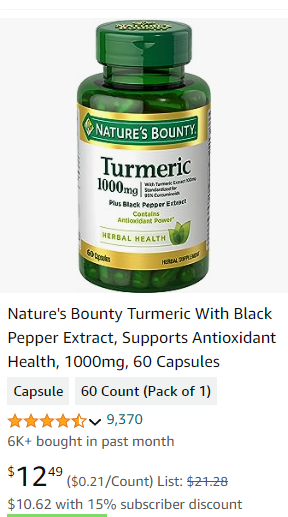
Example #3 Herb Turmeric
Choice #1: Off the shelf: $12.49/(1 gm x 60) = $0.21 / gram
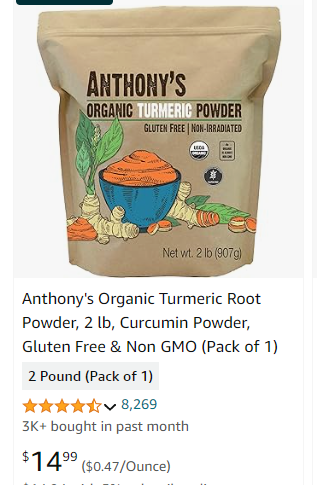
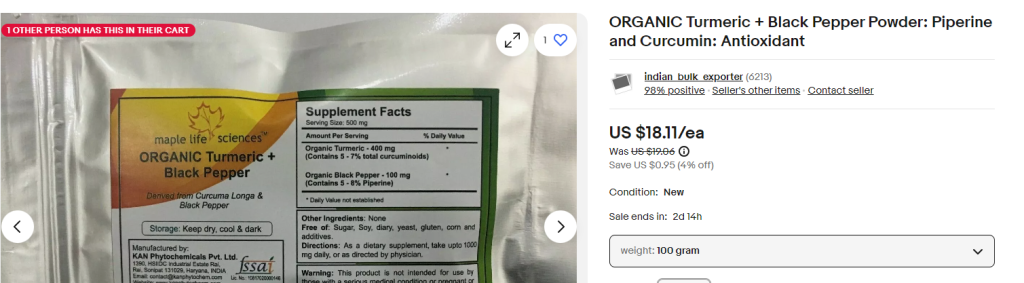
Choice #2: Bulk – from Amazon (note this is Organic, above is not): $14.99 / 907g = $0.016 / gram
Bottom Line: Up to 90% reduction in Supplement Costs is possible
There are always other factors — for example, some probiotics may only be available from just one supplier (i.e. L. Jensenii, E. Coli Nissle 1917). Do you want it to be Organic? Degree of trust in manufacturer, supply chain handling, seller’s handling (I deemed it very unlikely that Probiotics sold by Amazon are refrigerated, more likely just sit in their warehouses until sold).
Remember: Most supplements are high profit margins. At least one supplement seller who also sells microbiome testing kits is suspected to sell their kits at below cost because of the profit from selling the supplements to the same customers.
Our own experience with Maple Life Sciences probiotics have been awesome. We see changes in stools within 48 hours when we rotate between probiotics.