Overall cholesterol has been reported normal with CFS, but HDL (the good cholesterol) is significantly low. This can result in MDs doing symptom/lab results treatment instead of addressing the root cause.
- “Plasma lathosterol was decreased in both males and females with CFS (Tables 2 and and3).3). Total plasma cholesterol, desmosterol, cortisol, and aldosterone were normal in both males and females with CFS….Our data are consistent with increased flux through the desmosterol pathway to maintain normal cellular levels of cholesterol. The desmosterol pathway corresponds to the stress-inducible arm of de novo cholesterol and sterol synthesis.” [2016] While total cholesterol was normal, the mechanism of production was not.
- “Plasma chenodeoxycholic acid (CDCA) was decreased in females (Table 3, Females). CDCA is a primary bile acid made from cholesterol. Decreased cholesterol flux can result in decreased substrate for bile acid synthesis needed for normal fat digestion and microbiome signaling (24). The absence of adequate bile acid delivery can lead to a loss in intestinal mucosal integrity and leaky gut via a cascade of events stemming in part from disrupted farnesoid X receptor signaling”
- “These facts suggest that CFS is an evolutionarily conserved, genetically regulated, hypometabolic state similar to dauer that permits survival and persistence under conditions of environmental stress but at the cost of severely curtailed function and quality of life.” – except the stress in this case is caused by bacteria shifts.
- “The CFS group had higher levels of triglycerides (p = 0.03), MDA (p = 0.03) and CO (p = 0.002) and lower levels of HDL cholesterol (the good cholesterol) (p = 0.001) than the control group. There were no significant differences in the levels of total protein, total cholesterol or LDL cholesterol...The CFS group had an unfavorable lipid profile and signs of oxidative stress induced damage to lipids and proteins. ” [2012]
- “a control group of 40 healthy women and 40 CFS women. Levels of total cholesterol (TC), triglycerides (TG), LDL cholesterol (LDLc), HDL cholesterol (HDLc), and malondialdehyde (MDA) levels were measured. There was a negative correlation between HDLc and MDA levels (r=0.3; P=.046), a positive correlation between TG and MDA levels (r=0.4; P=.006), and lower levels of HDL cholesterol in the CFS group (P=.036). [2010]
- “Bacteroidetes showed positive correlation with LDL- and HDL-cholesterol levels, whereas Firmicutes showed negative correlation with total cholesterol, LDL- and HDL– cholesterol.” [2016]
Concurrent Treatment
Or should I say, how to help correct the shift of bacteria and improve HDL cholesterol. There were sufficient human studies to just use those.
“Recent population-based association studies have shown that the gut microbiota composition can explain a substantial proportion of the inter-individual variation in blood triglycerides and HDL-cholesterol level and predict metabolic response to diet and drug.” [2016]
- Almond Oil – “almond oil elevating the levels of so-called ‘good cholesterol’, high-density lipoproteins (HDL), whilst it reduces low-density lipoproteins (LDL).” [2010] I suspect eating almonds may be as good or better.
- ” replaced half of their habitual fat (approximately 14% of approximately 29% energy) with either whole almonds (WA) or almond oil (AO) for 6-wk periods… whereas HDL cholesterol increased 6%.” [2002]
- The use of probiotic L. fermentum ME-3 containing Reg’Activ Cholesterol supplement for 4 weeks has a positive influence on blood lipoprotein profiles and inflammatory cytokines: an open-label preliminary study[2016]. “HDL cholesterol level rose from 1.60 to 1.67 mml/l,” i.e. 4%.
- “a probiotic containing… L. Casei, B.Bifiudu and L. Fermentum .. significantly increased HDL-cholesterol levels (2.7 from 0.9 ) compared with the placebo after 12 weeks.” [2016] – a 200% increase in HDL.
- “Previous clinical studies have reported mixed results regarding the effect of probiotics on lipid metabolism…Subjects treated with probiotics demonstrated reduced total cholesterol and LDL cholesterol compared to control subjects by 7.8 mg/dL (95% CI: -10.4, -5.2) and 7.3 mg/dL (95% CI: -10.1, -4.4), respectively. There was no significant effect of probiotics on HDL cholesterol or triglycerides.” [2015] L. Fermentum appears not to be included in this review.
The Gut Microbiome Contributes to a Substantial Proportion of the Variation in Blood Lipids [2015].
- “we identified 34 bacterial taxa associated with body mass index and blood lipids; most are novel associations. Cross-validation analysis revealed that microbiota explain 4.5% of the variance in body mass index, 6% in triglycerides, and 4% in high-density lipoproteins, independent of age, sex, and genetic risk factors. A novel risk model, including the gut microbiome explained ≤ 25.9% of high-density lipoprotein (HDL) variance, significantly outperforming the risk model without microbiome. Strikingly, the microbiome had little effect on low-density lipoproteins or total cholesterol.”
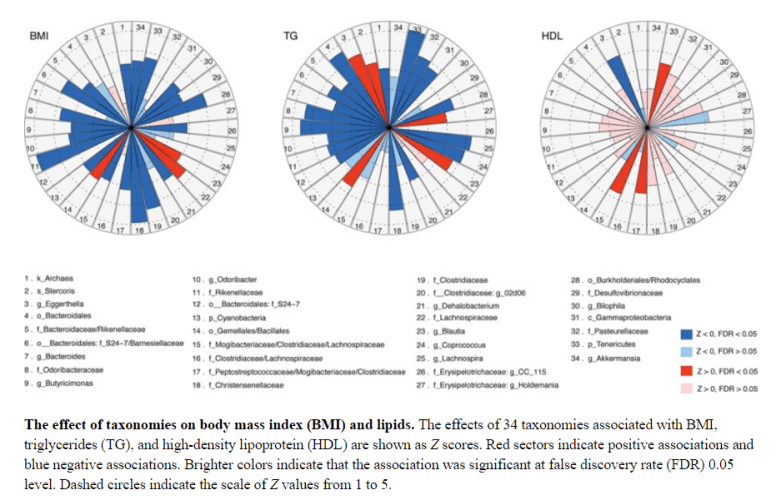
“Akkermansia , Christensenellaceae (phylum Firmicutes; N18) and the phylum Tenericutes and higher levels of HDL (P=0.0047 and P=0.0006, respectively) [RED in chart above]… genus Eggerthella (N3) with decreased HDL (P=6.3×10−5), [BLUE in chart above]”
“We observed that the gut microbiome makes a significant contribution, beyond that of clinical risk factors and genetics, to the individual variance seen in BMI and to the blood levels of triglycerides and HDL,but that it has little effect on LDL or TC levels. ”
Bottom Line
While the bacteria cited above are not currently available as a probiotics, we do have L. Fermentum available as a probiotic that has significant effect after 4 weeks and major effect after 12 weeks. Adding almonds as a regular part of your diet would also help.