IBS is a common morbidity for both ME/CFS and Long COVID. This is reported often in samples, and thus being examined if it reaches our threshold for inclusion as defined in A new specialized selection of suggestions links. It does, but the degree of association (z-scores) are lower than prior special studies despite having a larger study population.
Study Populations:
| Symptom | Reference | Study |
| ME/CFS with IBS | 1111 | 53 |
- Bacteria Detected with z-score > 2.6: found 190 items, highest value was 8.4
- Enzymes Detected with z-score > 2.6: found 182 items, highest value was 6.3
- Compound Detected with z-score > 2.6: found ZERO items
The highest z-scores above are greater than other symptoms despite smaller sample size. This indicates that the causes have more of a signature and thus more homogeneous bacteria shifts then ME/CFS without IBS.
Interesting Significant Bacteria
All bacteria found significant had too low levels. Many Bifidobacterium species are significant
| Bacteria | Reference Mean | Study | Z-Score |
| Sporolactobacillus (genus) | 172 | 36 | 8.4 |
| Sporolactobacillus putidus (species) | 172 | 36 | 8.4 |
| Sporolactobacillaceae (family) | 170 | 36 | 8.3 |
| Bifidobacterium kashiwanohense PV20-2 (strain) | 319 | 56 | 6.7 |
| Bifidobacterium catenulatum subsp. kashiwanohense (subspecies) | 309 | 56 | 6.6 |
| Blautia wexlerae (species) | 6022 | 3373 | 6.1 |
| Bifidobacterium gallicum (species) | 3699 | 631 | 6 |
| Bifidobacterium cuniculi (species) | 80 | 22 | 6 |
| Bacteroides finegoldii (species) | 2729 | 550 | 5.6 |
| Desulfovibrio simplex (species) | 219 | 51 | 5.4 |
| Succinivibrio dextrinosolvens (species) | 986 | 88 | 5.3 |
| Escherichia (genus) | 6011 | 1167 | 5.2 |
| Phocaeicola sartorii (species) | 820 | 317 | 5.1 |
| Haemophilus parahaemolyticus (species) | 66 | 20 | 5.1 |
| Lactiplantibacillus pentosus (species) | 123 | 28 | 5 |
| Clostridium chartatabidum (species) | 302 | 50 | 5 |
| Phocaeicola massiliensis (species) | 13851 | 4358 | 5 |
Interesting Enzymes
All enzymes found significant had too low levels.
| Enzyme | Reference Mean | Study Mean | Z-Score |
| (2S)-3-(4-hydroxyphenyl)-2-isocyanopropanoate,2-oxoglutarate:oxygen oxidoreductase (decarboxylating) (1.14.20.10) | 131 | 21 | 6.3 |
| (2S)-3-(4-hydroxyphenyl)-2-isocyanopropanoate,2-oxoglutarate:oxygen oxidoreductase (1.14.20.9) | 131 | 21 | 6.3 |
| propanoyl-CoA:oxaloacetate C-propanoyltransferase (thioester-hydrolysing, 1-carboxyethyl-forming) (2.3.3.5) | 1438 | 425 | 5.3 |
| L-tyrosine:D-ribulose-5-phosphate lyase (isonitrile-forming) (4.1.99.24) | 103 | 32 | 5.3 |
| L-pipecolate/L-proline:NADP+ 2-oxidoreductase (1.5.1.21) | 177 | 47 | 5.2 |
| (R)-lactate hydro-lyase (4.2.1.130) | 1514 | 326 | 5.1 |
| L-carnitinyl-CoA hydro-lyase [(E)-4-(trimethylammonio)but-2-enoyl-CoA-forming] (4.2.1.149) | 1371 | 328 | 5.1 |
| acyl-CoA,ferrocytochrome b5:oxygen oxidoreductase (6,7 cis-dehydrogenating) (1.14.19.3) | 1009 | 261 | 5.1 |
| (2S,3R)-3-hydroxybutane-1,2,3-tricarboxylate pyruvate-lyase (succinate-forming) (4.1.3.30) | 1389 | 431 | 5 |
| CMP-N-acetyl-beta-neuraminate:beta-D-galactoside alpha-(2->6)-N-acetylneuraminyltransferase (configuration-inverting) (2.4.99.1) | 66 | 20 | 5 |
| glutarate, 2-oxoglutarate:oxygen oxidoreductase ((S)-2-hydroxyglutarate-forming) (1.14.11.64) | 1232 | 316 | 5 |
Cross Validation
Looking at Medical Conditions with Microbiome Shifts from US National Library of Medicine we see agreements on many items (note that we have more bacteria identified because we have bigger sample sizes than those studies). Note that Escherichia (genus) is low, as was reported in the first study of the microbiome from Australia in 1998.
For the very few studies on ME/CFS with IBS
- Bifidobacterium (genus)
- Coprococcus catus
For studies of Irritable Bowel Syndrome 📚, we have agreement of these 7 bacteria
| Bacteria | Z-Score | Direction |
| Bacillus (genus) | 2.1 | L |
| Bifidobacterium (genus) | 2.4 | L |
| Methanobrevibacter smithii (species) | 4.3 | L |
| Phocaeicola vulgatus (species) | 2.8 | L |
| Sutterellaceae (family) | -2.3 | H |
| Turicibacter (genus) | 2.9 | L |
| Veillonella (genus) | 3.3 | L |
For studies on Inflammatory Bowel Disease 📚, we have agreement on these
| Bacteria | Z-Score | dIRECTION |
| Bacteroides fragilis (species) | 2.5 | L |
| Bacteroidetes (phylum) | 2.1 | L |
| Bifidobacterium (genus) | 2.4 | L |
| Cyanobacteria (phylum) | 2.8 | L |
| Methanobrevibacter smithii (species) | 4.3 | L |
| Prevotella copri (species) | 3 | L |
Bottom Line
The key take away is that Bifidobacterium levels appears to be a significant contributor. Lactobacillus is NOT (and likely is a contributor to oversupply of lactic acid causing brain fog). READ THE LABEL OF YOUR PROBIOTICS — you want Bifidobacterium without Lactobacillus.
The second probiotic to take is any of the E.Coli probiotics: Mutaflor (only available in a few countries) or Symbioflor-2 (US Source, World Wide Source) . NOTE: Lactobacillus is hostile to E.Coli, a second reason to avoid those probiotics.
A Priori suggestions are now available:
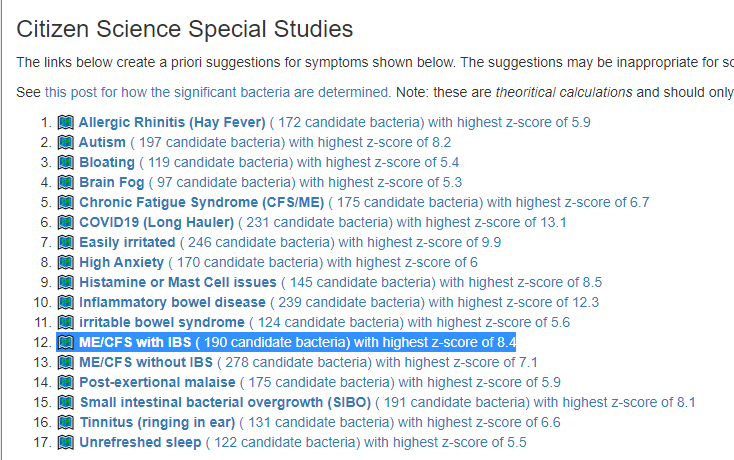
The top items are below (more on the web page). Remember no microbiome will be an exact match and these lists may contain items to avoid; using your own microbiome data is always the best choice. As always, any changes should be reviewed by your MD before starting.