
The core of my model is a significant shift of the microbiome due to some event that does not return to normal after the event. Details include the same general pattern of shift (no bifidobacteria, lactobacillus, E.Coli coupled with overgrowth of bacteria hostile to them).
Research Suggesting They were the same
- Chronic fatigue in Gulf War veterans: should it be treated as chronic fatigue syndrome? [2009]
- Chronic fatigue syndrome in male Gulf war veterans and civilians: a further test of the single syndrome hypothesis [2008].
Coagulation Pattern
“Most symptoms of Gulf War Illness (GWI) are similar to Chronic Fatigue Syndrome (CFS) and/or Fibromyalgia (FM). We investigated whether these symptoms are associated with an activated coagulation system as has been reported in some cases of CFS/FM. The coagulation assays include activation markers of the cascade, platelet activation and hereditary risk factors. Our findings show activation of the coagulation system in GWI. This evidence of a hypercoagulable state suggests that symptoms may be due to poor blood flow and, therefore, a basis for the potential utility of anticoagulant therapy.” [2000]
- “There appears to be significant overlap, in the symptoms of Gulf War Illness, CFS and Fibromyalgia “
- “The symptoms of CFS/FM and GWI are very similar. The positive ISAC testing of the GWI patients parallels the results seen in CFS/FM patients. The hereditary risk profile is also positive in both. GWI may be a unique subset of CFS/FM.”
NOTE: my model has the metabolites (chemicals) produced by bacteria overgrowth triggering coagulation in those susceptible due to DNA.
Mycoplasma Model of Prof. Garth Nicholson
“They identified the causal pathogen for Gulf War syndrome as Mycoplasma fermentans, which was a different strain from the natural pathogen, raising the possibility that it was man-made biological weapon. They successfully treated patients with multiple courses of specific antibiotics, such as doxycycline, ciprofloxacin, azithromycin, clarithromycin or minocycline.” [Wikipedia]
Note: The antibiotics (treatment) are the same ones that I advocate for correcting the microbiome.
GWI Microbiome
“upper GI section samples revealed a significant increase in the Bacteroidetes and a significant reduction in Bifidobacterium No significant changes were detected in
the load of Firmicutes and Desulfovibrio. In lower GI section samples, Bacteroidetes were dominant in both control and GWI groups (control: 19.50 +/- 0.62, GWI: 19.60 +/- 0.46) compared to other phyla. MiSeq-derived results also showed that in samples from the upper GI section, the contribution of Bacteroidetes was more pronounced in GWI patients compared to controls. ….Conclusion: The composition of the microbial community in the small intestine is different in patients with GWI than controls supporting the idea of shift in the microbiome in GWI.” [2014]
A 2017 study states “With sufficient evidence from GW veteran studies about the existence of chronic fatigue and GI disturbances coupled with neuronal inflammation, it is all the more important that we explore newer and novel mechanistic pathways, especially the role of the gut microbiome in modulating adverse outcomes in GWI such as neuroinflammation and intestinal injury”
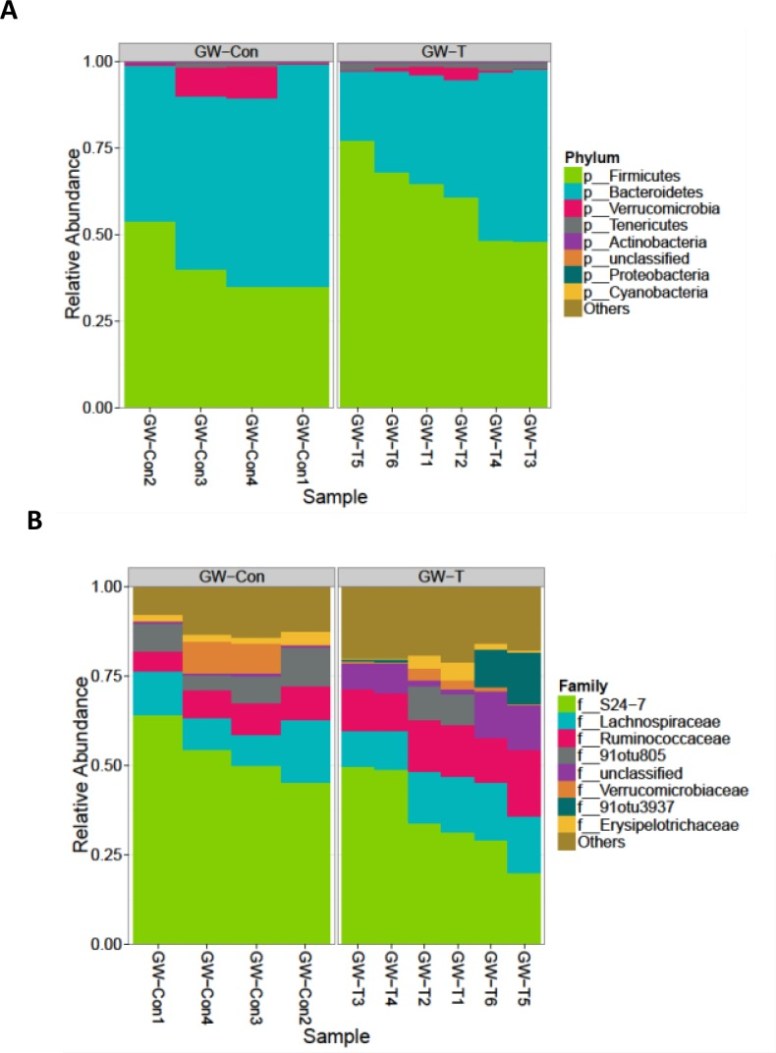
The diagrams below showed the changes of gulf war chemical exposed group (GW-T) versus control group fed with vehicle (GW-Con). Increase of firmicutes and decrease of bacteroidetes.
Bottom Line
Studies of GWS have dropped off, but it appears that the microbiome is now being considered. My expectation is that it will overlap with CFS, possibly with less divergence than that seen in CFS.
