
Melatonin has often been mentioned in my posts, without a deep dive into it.
“Melatonin, also known as N-acetyl-5-methoxy tryptamine,[1] is a hormone that is produced by the pineal gland in animals and regulates sleep and wakefulness” [Wikipedia]
- “Serum melatonin levels of FMS patients were not statistically different from those of controls (P > 0.05).” [2013]
- ” FMS patients have lower melatonin secretion during the hours of darkness than the healthy subjects.” [2011]
- “Agomelatine treatment, but not melatonin, was associated with a significant reduction of perceived fatigue and an increase in perceived quality of life.”[2014]
- “Using melatonin (3 mg or 5 mg/day) in combination with 20 mg/day fluoxetine resulted in significant reduction in both total and different components of FIQ score compared to the pretreatment values.” – but melatonin alone was not. [2011]
- Therapy of circadian rhythm disorders in chronic fatigue syndrome: no symptomatic improvement with melatonin or phototherapy [2002].
The more likely cause of sleep disorders with CFS/FM/IBS is hypoxia (low oxygen) which is known to cause severe sleep problems. Melatonin can help with that, but other oxygen delivery items should be considered too.
- “melatonin has no effect on trophoblast cells in normoxic state but restores the redox balance of syncytiotrophoblast cells disrupted by hypoxia/reoxygenation. ” [2016]
- Hypoxia-induced vascular endothelial growth factor secretion by retinal pigment epithelial cells is inhibited by melatonin via decreased accumulation of hypoxia-inducible factors-1α protein [2016].
On the flip side, there some some bacteria that are associated with a lack of sleep: Partial Sleep Deprivation. On DataPunk.Net we read:
ENHANCES:
INHIBITS:
In other words, it contributes to a shift of the firmicutes/bacteroidetes ratio.
- ” in particular through [Melatonin] ability to decrease the Firmicutes-to-Bacteroidetes ratio and increase the abundance of mucin-degrading bacteria Akkermansia, which is associated with healthy mucosa. ” [2017] – Checking Akkermansia levels first (most are low, but a few are high).
- Optimal dosages for melatonin supplementation therapy in older adults: a systematic review of current literature[2014].
- “The mean age varied from 55.3 to 77.6 years. Melatonin dosage varied from 0.1 mg to 50 mg/kg and was administered orally in all studies.”
Bottom Line
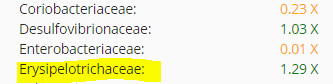
If someone has a high firmicutes/bacteroidetes ratio (i.e. firmicutes > 1.2x and /or bacteroidetes < .8x) then melatonin is a reasonable supplement, especially if there is overgrowth of Coriobacteriaceae or Erysipelotrichaceae. This applies to a subset of CFS patients.
Example:
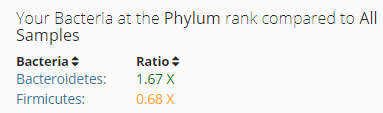
On the Family Level
The dosage is unclear. The literature reports: “0.1 mg to 50 mg/kg “, so for 100 lb individual:
- 4.5 mg/day to
- 2 gram/day
“For trouble falling asleep: 0.3 to 5 mg of melatonin daily for up to 9 months has been used. For sleeping problems in people with sleep-wake cycle disturbances: 2 mg to 12 mg taken at bedtime for up to 4 weeks has been used.” [WebMD]
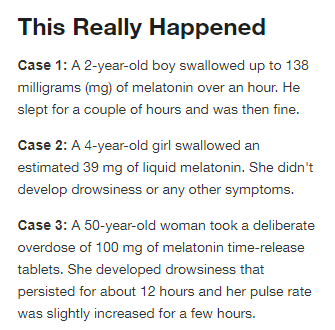
Poison Control reports:
“307 articles were elicited and 9 were related to Melatonin adverse effects. The range of MLT dose involved in the adverse reactions oscillated between 1 mg and 36 mg. The adverse reactions were: one patient with autoimmune hepatitis, one case of confusion due to MLT overdose, one case of optic neuropathy, four subjects with fragmented sleep, one psychotic episode, one case of nistagmus, four cases of seizures, one case of headache and two cases of skin eruptions.” [2001]
As always, consult with your medical professional before starting or altering your supplements.
