A SIBO patient shared with me their uBiome results. Before I look at them I will state a question that I have:
- Is SIBO substantially the same dysfunction but the person’s DNA can handle it without CFS or FM symptoms? We know that many symptoms are associated with specific SNP for both syndromes….
Patient Background
“After a bad case of food poisoning, I ended up with SIBO. The food poisoning was from campylobacter which produces the cdtb toxin…In my case of SIBO, it was caused by an autoimmune response. Taking probiotics triggers SIBO symptoms but I know I need to fix this imbalance. I would love to hear your thoughts or you can wait until I get my second results (unless you have some probiotics to try before retesting).”
Basic Criteria for CFS/FM


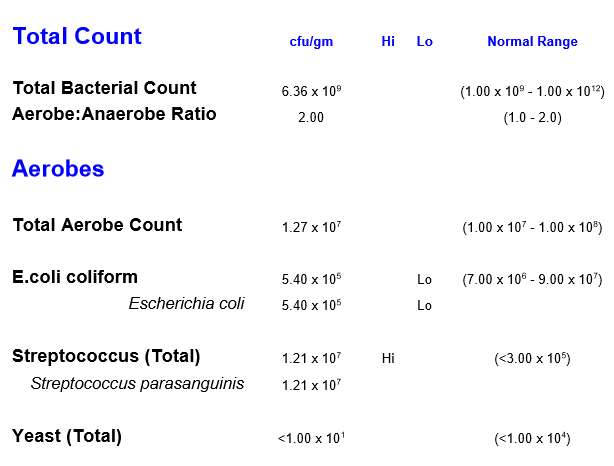
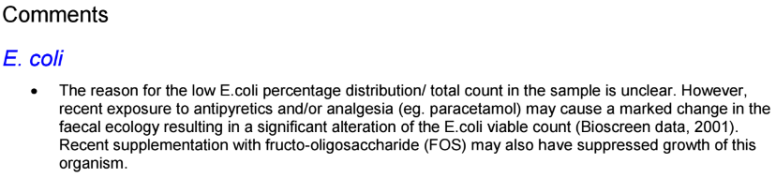
Lowish E.Coli
- Not directly reported, but it parent is: Enterobacteriaceae which is 13% of the reference group
What seems different from the usual CFS profile is that the Firmicutes/Bacteroidetes ration is effectively normal — a significant difference.

- Diversity: 59%ile – usually CFS is very high (95+%ile)
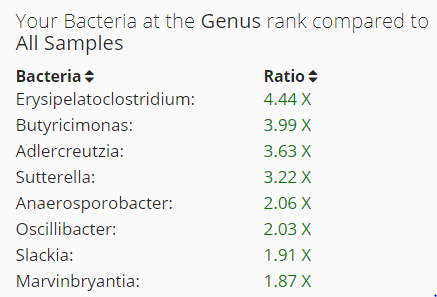
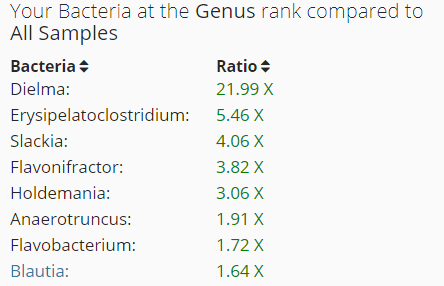
Overgrowth of Bacteria Genus
My criteria is to look at only those that are 1.5x or higher. We have only 2, a lot less than those seen in CFS/FM.
Rare Bacteria

Analysis of Over Growth
As usual, I head to datapunk.net to speed analysis (and allow folks to check or extend my research).
- Dielma (genus)
- Erysipelatoclostridium (genus)
- Slackia (genus) – no info
- Holdemania (genus)
- Anaerotruncus (genus)
- Flavonifractor (genus)
- Blautia (genus) High
- Salmonella (genus) Rare
- Vagococcus (genus) Rare
- Delftia (genus) Rare no info
- Citrobacter (genus) Rare
The numbers above are used below
NUTRIENTS/ SUBSTRATES
INHIBITED BY
- Flaxseed – 1,2, 4, 7
Walnuts – 5, 7- Curcuma longa – 8
- Aloe vera – 8
- Plantain bananas – 8
- Garlic (allicin) – 8
- Pomegranate ellagitannins – 8, 11
- Sarcodiotheca gaudichaudii (red seaweed) – 8
- Hyocyamine – 8
- Butyrate -5
- Acetic acid – 5
- Proton-pump inhibitors – 4
ENHANCED BY
- Partial Sleep Deprivation – 1,2, 4
- Aspartame – 11
- Berberine – 7
- Cholic acid – 7
- Resistant starch (type IV) -7
Walnuts – 5, 7- Resistant starch (type II) -7
- Saccharomyces boulardii – 7
- Gallate – 5
- Chemotherapy – 4
INHIBITS
- Bifidobacterium – 1, 4, 5, 7, 8, 11
Bottom-Line
This SIBO person has a uBiome very close to CFS/FM patients but with one, possibly critical, difference: Firmicutes/Bacteroidetes is normal. Also the diversity is normal.
While this is a single uBiome from SIBO without CFS, it suggests that the transition from SIBO to CFS may be caused by the Firmicutes/Bacteroidetes being lost; with this lost the equilibrium is gone and a ton of other bacteria genus can move in — pushing diversity to the top.
Suggestions for the patient to discuss with their medical professional:
- Having flaxseed with porridge daily
- Taking butyrate supplements, possibly taking the Miyarisan (Clostridium butyricum) probiotic.
- The Partial Sleep Deprivation suggests melatonin supplements
- I would not recommend Proton-pump inhibitors because so many of the bacteria seen in CFS are enhanced with PPIs.
- Reducing glucose in the diet. This is a specific type of sugar — regular sugar is converted to glucose which makes these high bacteria dependent on other bacteria. Having glucose in foods eliminates this dependency and allows more rapid growth.
- This means going to NutritionData.Self.com listing high glucose foods and reducing them. This is not a low sugar diet suggestion, but a low glucose diet (a specific type of sugar).
Probiotics: I would suggest trying at least one from each of the following two groups, I suspect the patients have done just the usual lactobacillus ones.
- Soil Based Organisms
- E-Coli Probiotics
As always — for educational purpose only.
Hypothesis
SIBO is the lost of Bifido, Lactobacillus, E.Coli without a loss of the Firmicutes/Bacteroidetes balance and without the blossoming of additional species (i.e. normal diversity)
CFS is the lost of Bifido, Lactobacillus, E.Coli with a loss of the Firmicutes/Bacteroidetes balance and with the blossoming of additional species (i.e. high diversity)