
I had done an analysis of his original before doing deep-dives in this Aug, 2017 post and a followup post later that month.
Reminder: This is all based on a model, a hypothesis that appears to match the known studies. The model purpose is to increase the odds of getting improvements. There are many factors that may influence what works and does not work – DNA, specific strains of some bacteria. We do not have enough knowledge to know what will work for any individual — we can make suggestions that appear to be far more probable to work.
Reader Notes
First, Thank you for all the work you do that so benefits this community.
Standard Items:
- Lactobacillus: 0.04x ( 0.04 Prior)
- Bifidobacterium: < 0.01 (< 0.01 Prior)
- Akkermansia: 1.98x (7.36x prior)
- Diversity: 68%ile (95%ile prior)
- Firmicutes to Bacteroidetes: 1.0:1 (Normal 2.1:1)
- 1.1:1 prior
- Bacteroidetes 1.25 –> 1.5
- Firmicutes 0.64 –> 0.7
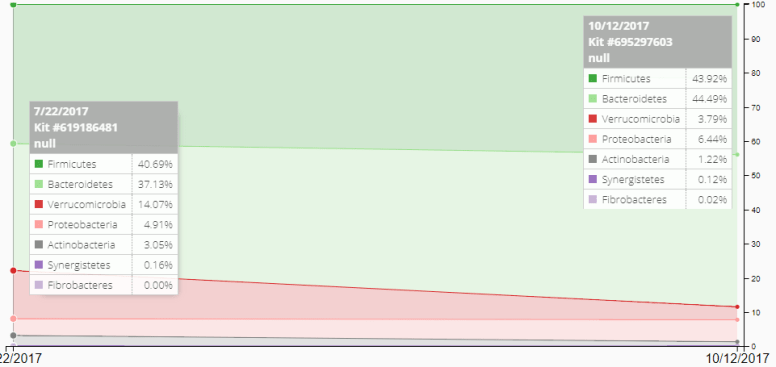
Historic Trends
We can see there are significant shifts of some phylums
Uncommon Bacteria
| Proteiniphilum | Genus | 0.7% |
| Caldicoprobacter | Genus | 3.1% (was in Prior) |
| Parasporobacterium | Genus | 3.5% |
| Parvibacter | Genus | 4.1% (was in Prior) |
| Christensenella | Genus | 4.5% |
High Bacteria
|
Bacteria
|
Ratio
|
|---|---|
| Oscillospira: | 4.19 X (2.42x prior) |
| Alistipes: | 3.54 X (4.53x prior) |
| Parasutterella: | 2.50 X (2.98x prior) |
| Coprobacter: | 2.15 X |
| Intestinimonas: | 2.14 X (2.00x prior) |
| Butyricimonas: | 2.05 X (1.92 prior) |
| Thalassospira: | 1.90 X |
| Flavonifractor: | 1.60 X |
| Pseudobutyrivibrio: | 1.55 X |
Following have dropped below 1.5x
Akkermansia (was 5.26x –> down to 1.42): , Intestinibacter (was 5.0x –> down to 0.24x):
References
- Oscillospira: https://cfsremission.wordpress.com/2017/10/15/decreasing-oscillospira-genus/
- Alistipes: https://cfsremission.wordpress.com/2017/10/09/decreasing-alistipes-genus/
- Parasutterella: https://cfsremission.wordpress.com/2017/10/19/decreasing-parasutterella-genus/
- Coprobacter: https://cfsremission.wordpress.com/2017/11/06/decreasing-coprobacter-genus/
- Intestinimonas: https://cfsremission.wordpress.com/2017/11/05/reducing-intestinimonas-genus/
- Butyricimas: https://cfsremission.wordpress.com/2017/10/14/decreasing-butyricimonas-genus/
- Thalassospira: https://cfsremission.wordpress.com/2017/10/22/reducing-thalassospira-genus/
- Flavonifractor: https://cfsremission.wordpress.com/2017/11/05/reducing-flavonifractor-genus/
- Pseudobutyrivibrio: https://cfsremission.wordpress.com/2017/10/15/decreasing-pseudobutyrivibrio-genus/
Bottom Line Suggestions For New Ones
The lists below are done by merging the lists from the deep dives linked above. Some items may encourage one genus and discourage another genus — those are removed (unless it seems that it strongly predominates on one). The impact on Lactobacillus, Bifidobacterium and E.Coli are intentionally ignored [See this post for the logic]. This is all based on applying logic to the results of studies — thus theoretical. This is an addition (not a replacement) to this overview post.
Avoid
- Barley and oat
- Bifidobacterium animalis subsp. lactis B-12®
- Bifidobacterium catenulatum
- Bifidobacterium pseudocatenulatum
- Black Tea
- Clostridium butyricum (i.e. Miyarisan) probiotics
- Generic Bacillus probiotics
- Lactobacillus fermentum
- Lysine supplements and foods
- Metformin
- Saccharomyces boulardii
- Vitamin K2
- Walnuts
Take
- Alchohol
- Bacillus subtilis natto
- Bifidobacterum Bifidum
- Bifidobacterum Infantis
- Cranberry bean flour (or fresh cranberries)
- E.Coli Probioitics
- Enzymatically modified resistant starch
- Faecalibacterium prausnitzii
- Flaxseed
- Gallate – Green Tea
- Inulin
- Lactobacillus Casei
- Lactobacillus kefiri LKF01
- Lactobacillus paracasei
- Lactobacillus salivarius
- L-glutamine
- Polymannuronic acid
- Resistant starch (type II & IV)
- Tannin and Gallate — green tea see this web page.
Personal Comments
It is interesting that Black Tea is a to avoid, while Green tea is a to take.
This is an education post to facilitate discussing this approach with your medical professionals. It is not medical advice for the treatment of any condition. Always consult with your medical professional before doing any changes of diet, supplements or activity. Some items cites may interfere with prescription medicines.
