
A reader wrote me because of progress with medical professionals have not happen and there have been significant apparent side-effects from
“on the that meeting with the doctor I discussed my parasitic infection with blastocystis hominis, and the s.boulardii treatment so he prescribed to me OMNIFLORAN ( (Lactobacillus gasseri and Bifidobacterium longum) & Perenterol Forte. (Saccharomyces cerevisiae)
What does the literature report?
I cannot advise what a reader should do, such must come from medical professionals. What I can do is simple report what is in the literature (with links to the literature) for educational purposes.
- “Blastocystis hominis, previously considered a harmless yeast, is now classified as a protozoan inhabiting the human intestinal tract. The pathogenicity of B. hominis remains controversial and is currently the subject of extensive debate. As a result of the uncertainty surrounding the pathogenic role of B. hominis, large-scale treatment trials of B. hominis infection have so far been lacking. In spite of this, several drugs have been reported to be active against the parasite.” [2003]
- “Because of this vast diversity, it has been suggested that the human parasite should no longer be referred to as Blastocystis hominis but instead should be called Blastocystis spp. or Blastocystis spp. subtype n (where n is the subtype number according to the Stensvold classification)” [2012]
- “There has been debate in the literature concerning the question of the pathogenicity of Blastocystis. Some studies suggest an association between the parasite and disease, but others do not [3, 18, 21]. “
- “A causal relationship has never been established for Blastocystis and diarrhea, and no reliable animal model exists, so Koch’s postulates have not been demonstrated for this organism. “
- “in some studies, Blastocystis was detected more frequently in patients with IBS than in a control group [27, 32, 35], whereas in other studies there was no association [18, 44]. “
- “Metronidazole is considered first-line treatment, but the success of eradicating Blastocystis with this drug has been reported to be anywhere from 0% to 100% [53]. “
- “Parasite infection by B. hominis is one of the most common diseases in our tropical medicine unit. Most patients are asymptomatic, or their symptoms can be attributed to other parasite infections. In those cases in which symptoms persist without being able to attribute them to other causes, a specific treatment is recommended.” [2018] i.e. a vacation to a tropical area, risks infection.
- “Parasitic stool testing in newly arrived refugees in Calgary, Alta.” [2017]. 30-40% has parasites. Since refugees often end up in food service, there is a risk that eating out risks infection.
- “In Poland, the subtypes ST1, ST2, ST3, ST4, ST6 and ST7 have been reported in humans so far. ” [2017] i.e. there are multiple types
- Low efficacy of metronidazole in the eradication of Blastocystis hominis in symptomatic patients: Case series and systematic literature review. [2017]
- Modulating the Gut Micro-Environment in the Treatment of Intestinal Parasites. [2016]
- “In fact, B. hominis is probably the most common protozoan detected in human faecal samples worldwide. Infection occurs in both immune-competent and immune-compromised individuals. Reported prevalence ranges from 2%–50% with the highest rates reported for developing countries with poor environmental hygiene. Infection appears to be more common in adults than in children “
- “An additional clinical study that administered S. boulardii or metronidazole showed potential beneficial effects in B. hominis infection relative to a reduction of symptoms and presence of parasites [19].”
- Clinical efficacy of Saccharomyces boulardii or metronidazole in symptomatic children with Blastocystis hominis infection.[2011] – 93+% cure rate in children with either reported. S. boulardii (250 mg twice a day,
Mayo Clinic
“If you have blastocystis without signs or symptoms, then you don’t need treatment. Mild signs and symptoms may improve on their own within a few days.
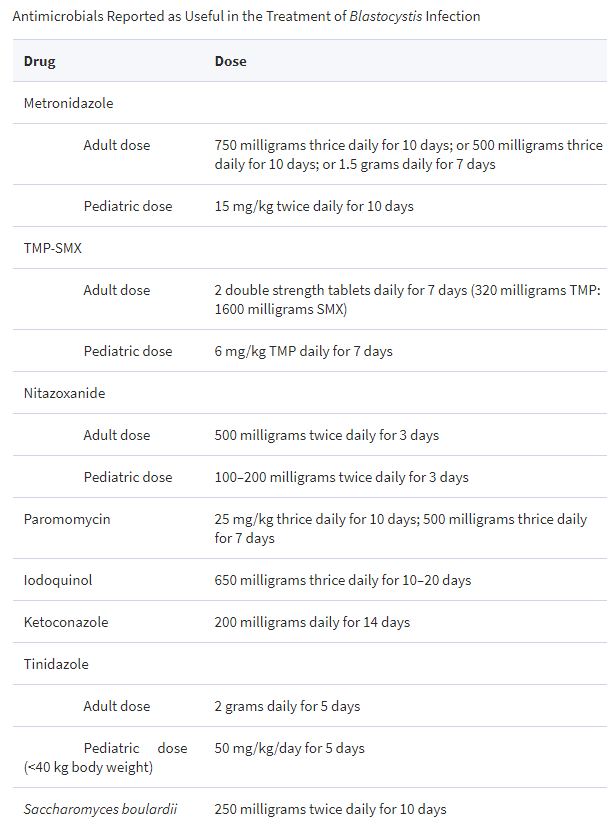
Potential medications for treating blastocystis infection include:
- Antibiotics, such as metronidazole (Flagyl) or tinidazole (Tindamax)
- Combination medications, such as sulfamethoxazole and trimethoprim (Bactrim, Septra, others)
- Antiprotozoal medications, such as paromomycin, or nitazoxanide (Alinia)
However, keep in mind that response to medication for blastocystis infection varies greatly from person to person. And, because the symptoms you’re having might be unrelated to blastocystis, it’s also possible that any improvement may be due to the medication’s effect on another organism.”
Bottom Line
There appears to be no firm evidence that blastocystis infections need treatment. It appears to be an opportunistic infection that simply grows as a result of other issues. Those other issues are what should be treated.
The reader took Saccharomyces cerevisiae (NOT Saccharomyces boulardii) for 10 days. I could find no literature that this probiotic is effective for blastocystis infections.
Saccharomyces cerevisiae impacts the microbiome also. I have nothing in my database on the impact of this on the microbiome. This reader also included her KyberKompact Pro report. The report showed the typical profile commonly seen:
- Low Lactobacillus
- Low Bifidobacterium
- Low Escherichia Coli
- Low Enterococcus spp.
- Low Faecalibacterium prausnitzii
- Low Akkermansia muciniphila
For S. Cerevisiae, I found:
- “Administration of S. cerevisiae RC016 caused the decline of a logarithmic unit for Enterobacteriaceae counts compared to the control.” [2016] – making the low Enterococcus worst.
- “SCB consumption positively influenced the establishment of the Porphyromonadaceae and Ruminococcaceae bacterial families in the colon. ” [2015]
Best suggestion moving forward:
- Get a uBiome done (simply because it gives more information!)
- Assume Enterococcus reduction is contributing to the symptoms.
See Enterococcus [genus] undergrowth for changes in diet that may help. Suggestions are:
- Bioflorin Enterococcus faecium SF 68
- Reservatrol (aka. Red Wine polyphenol)
- Sesame cake/Meal
- Buckwheat
- Navy and broad beans.
This is an education post to facilitate discussing this approach with your medical professionals. It is not medical advice for the treatment of any medical condition. Always consult with your medical professional before doing any changes of diet, supplements or activity. Some items cites may interfere with prescription medicines.
