Looking at the suggested probiotics, we find that MegasporeBiotic is a net -2.4 (Plus: 6, Negative: 8.4). An HU58 listed on the negative list. Given that she is very high in both of these… it makes sense.
Checking the modifiers, we see that this type of probiotic are indeed predicted to increase these two families.
FORGET about taking bifidobacterium and lactobacillus to increase bifidobacterium and lactobacillus . Take bacillus (which inhibits the inhibitors of bifidobacterium and lactobacillus )
I have added an educational page to the site. The purpose is to illustrate why focusing on a single bacteria may fail to produce results. You must also focus on the bacteria that support and contribute to it.
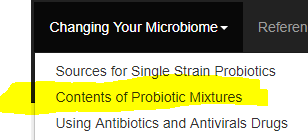
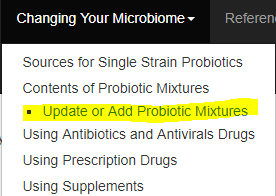
Where the new page is located
New button on the Available Samples Page
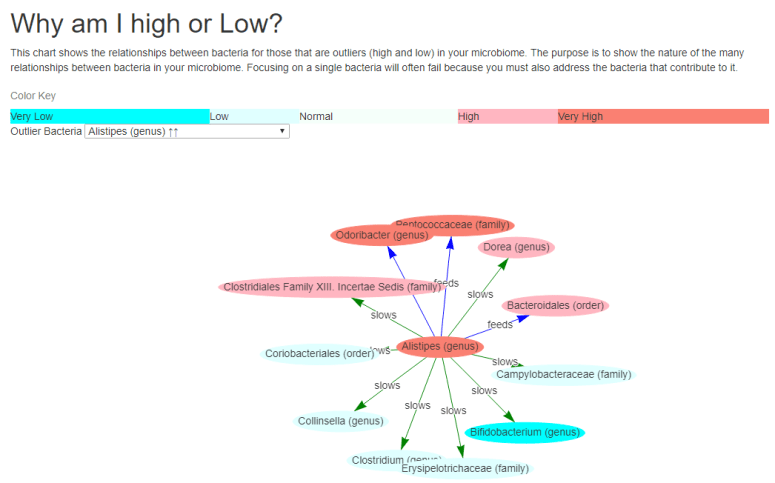
When you click this, a new page will appear as shown below
High bacteria slow other bacteria which may be low or very low
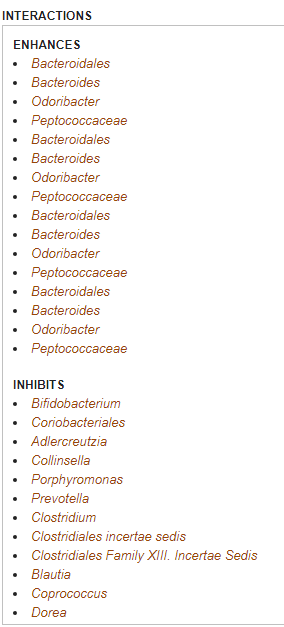
There are arrows pointing between the bacteria, labelled with their influence. Some examples;
High Alistipes slows / inhibits bifidobacterium. In this case, so very well that it is very low.
Alistipes feeds / encourages Odoribacter, Dorea, Peptococcaceae. so high amount of Alistipes results in higher amounts of these.
Alistipes also inhibits other bacteria… and we see many that are low.
To keep complexity down, I do not display bacteria in the middle range.
The Outliers list includes only the bacteria that are outliers AND which have known relationships with other bacteria.
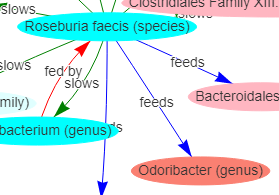
oseburia faecis is low, but Odoribacter is high! (read below for why)
A few things to remember:
A low bacteria may feed a bacteria that is very high. What this means is that OTHER things are feeding. For example, Roseburia faecis feed Odoribacter – so we would expect it to be low, but if you look above, we also see that Alisipes also feed it. Think of it this way: corn feed people, wheat feed people, barley feed people. If you have no corn, you may still have a lot of fat people.
Similarly, a high bacteria may feed other bacteria. Some of those may be low. To return to the food analogy: the bacteria may be producing pork — a lot of fat people, but none of them are Jewish or Vegetarians.
For those who do not have a ubiome sample available, I created a quick video showing the page.
I just finished coding it up this morning. The mixtures considered, are the mixtures that readers have entered. See this post on how to add them.
Step by Step
On the custom suggestions page you will see a new choice, automatically checked.
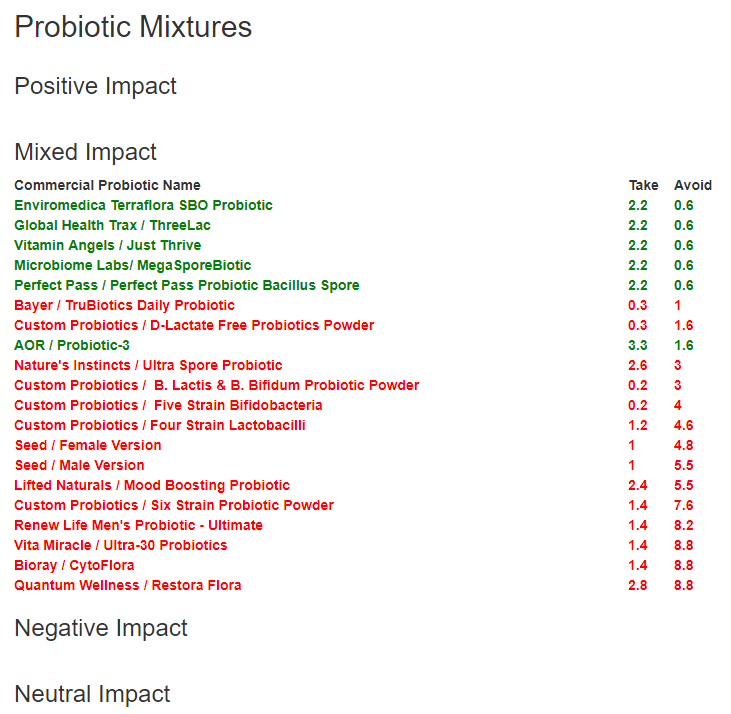
When you ask for suggestions, a new section will appear at the bottom.
Using my latest results — I am stopping Seed as a result.
Severe ME/CFS
I ran another person thru, and we got some definite takes
ME/CFS patient – severe
A Crohn’s Patient
Bottom Line
Dealing with probiotic mixtures is frustrating. Different areas of the world sell different mixtures and brand names. This new tool should allow easier objective evaluation.
At present suggestions on https://microbiomeprescription.com/ work by naming specific strains. This can often be a challenge to obtain for many readers. On the flip side, people will have a mixture and ask if they should take it.
The solution is to support mixtures:
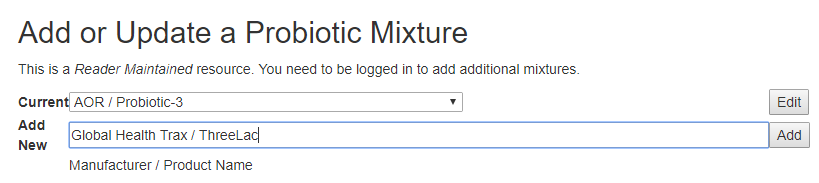
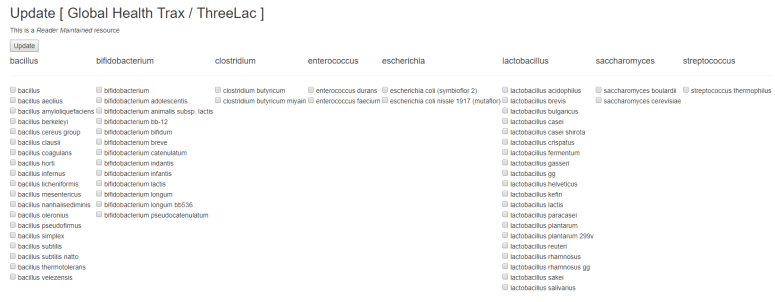
By allowing registered users to add probiotic mixtures
By having the suggestions review the mixtures and identify
good ones (some on the to take list, none on the to avoid list),
neutral ones (none on the to take or to avoid list) and
possibly risky ones (1 or more on the avoid list).
This post describes the first step.
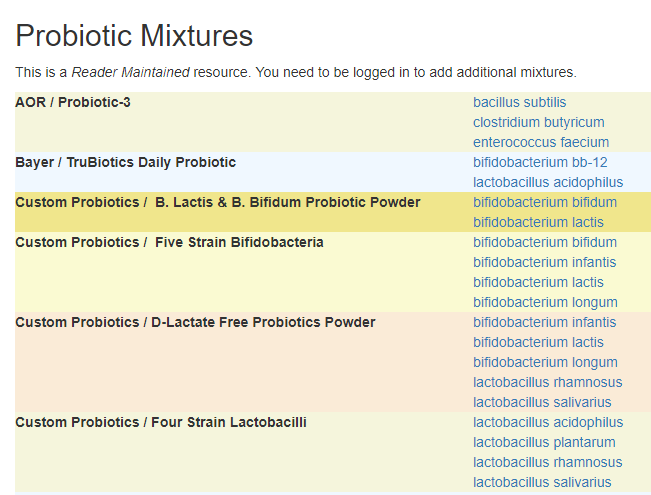
There are several new pages added today. First is a listing of probiotic mixtures
Some 6 years ago, I documented in a blog post a hypothesis that I had been using and felt sufficiently confidence about to commit to paper. I referenced an even earlier more speculative post from 2012.
” My best hypothesis on CFS is currently a stable dysfunctional microbiota (gut flora) that was triggered by an illness, poor diet, vaccination or chemical exposure. It is good to put this hypothesis to the test against prior successful treatments that resulted in some remissions. I have already looked at this in an earlier post, but thought a revisit on certain aspects would be good. “
Infection or even a single Phage changes the microbiome
Phages are specific hunters: each type kills just one type of bacteria. So when the scientists introduced a phage to the mice, they would see a decline in that type of bacteria. However, the impact on other bacteria was more surprising…. They found that when they introduced a phage to the mice and the bacterial composition changed, there were also changes in the levels of certain biologically active chemicals. If phages make sweeping changes to a mouse microbiome, they are likely to make changes in the human microbiome, too. The changes might be different, but the principle remains.
The effectiveness of any ME/CFS treatment depends on the microbiome
Some drugs work well for one person but are ineffective for another; some also produce adverse events for certain individuals but not others. A study, using human gut bacteria and a mouse model, investigates whether our gut bacteria might help explain why.
‘Using those data, they developed a mathematical model that successfully predicted the role of gut bacteria in metabolizing a second antiviral drug and clonazepam, an anti-seizure and anti-anxiety drug. The study found that the gut microbes were responsible for producing 20 to 80 percent of the circulating toxic metabolites derived from the three drugs.” The gut microbiome may be to blame for the toxic side effects some people experience from drugs that help many others, according to new research.11 Feb 2019
My earlier Eureka Post — found strong statistical relationships between many symptoms and bacteria.
Where Science is at and where I have leapt ahead
Science is just starting to accept the wide effect that bacteria has with the latest studies. In traditional scientific caution, it may take another decade before it is well accepted (look at the 30 years that it too for H. Pylori to be accepted as the cause of stomach ulcers).
Over the last six years, I have seen study after study come supporting my seven year old hypothesis. As more information came in, I moved on to accepting it and the logical consequence: we need to have approaches to modify / correct the gut bacteria. Unlike the usual bad bacteria infection, there is often no good or bad bacteria — rather too much of one and too little of another. Add to this that all of the bacteria interacts with each other.
If you go to DataPunk, and look at Dorea genus, you will see a long list of interactions with other bacteria… a very long list. Any change may have worst cascading effects!
Add to this already complex situation, the absence of research on what various drugs do — I recently try researching what the impact was of three different common histamines. I was lucky to find some material on one of them, the other two has unknown impact.
A reader recently shared this post from my long time friend, Cort Johnson
With my hypothesis, such a drug is likely to impact gut bacteria significantly. It turns out that there was a study on it’s impact and I had add it to my microbiome prescription site. Over 30 impacts. Whether it worked or did not work for a ME/CFS suffer would likely depend on their microbiome!
Suggestions are cutting edge science
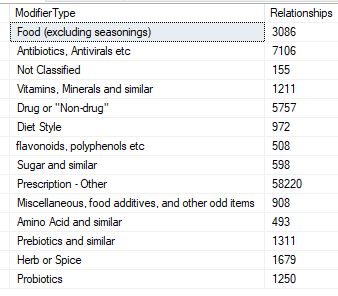
I have looked at many sites giving diet advice, even those connected with microbiome testing such as Thryve. The quality of the advice is effectively at general dietitian level, or naive using the microbiome (i.e. used a few studies only). The microbiome prescription site uses a database containing the following information:
The relationships are constantly being updated from new studies.
There was an interesting comment on my facebook page, something like “Correcting the microbiome have never been proven to cure any condition!” – absolutely correct, technically. BUT ALSO:
“There have never been a study published that showed that you can correct the microbiome” – In other words, the above comment was polemics.
My own experience (especially with the ongoing flare) is that you can correct the microbiome to some degree (totally normalize is a different question) and as you correct it, symptoms should reduce (as it has for me).
I know of no other resource, free or paid, that provides suggestions based on as many studies, considering as many factors as being produced by the microbiome prescription site. It may not be perfect, but it is probably more effective than the advice most MDs would hand out — which is often “Take a good quality probiotic” — whatever that means!
Bottom Line
After 7 years, trying a hypothesis, I am still using it and applying it. It holds water. It appears to work — but more importantly, it explains things. Using it and addressing some ‘black holes’ like histamines and mast cell issues are ongoing challenges. We are making progress.
“Hypotheses grow out of explaining empirical data.That is basic science.” Empirical data for me was the published reports of responses to various treatments for ME/CFS, as well as studies on the symptoms reported. All on PubMed or in conference reports. Most of the significant ones were published in 1998-2001.
The event that triggered my paying notice to the microbiome was during the 2010’s relapse — I could control all of the other symptoms with things like heparin, etc, herbs etc… but I never had GI issues before. As a result, I had filtered out all of the GI information looking at the literature. This event caused me to re-inspect the literature and lead to this hypothesis (after trying multiple others). It was far better at explaining all of the information and data then any other proposed at that time.