Patient Summary
– Current age 44
– Main symptoms: Brain fog, fatigue, weakness, exercise intolerance, feel worse after eating, certain weather (high winds or overcast skies) cause me to feel extremely anxious/exhausted. The physical symptoms haven’t changed much since teenage years, but are gradually worsening with age.
– Typically able to work around 10 hours per week, running own company from a zero-gravity chair, but requires significant effort. Brain fog is the major impediment.
– Hypersensitive to chemical fragrances, but equally sensitive to light, sounds, tastes, and touch. No strong Aspergian tendencies, but an INTJ on Myers-Briggs and a 5w4 on the Enneagram.
– Fell from the second floor to the first floor of family home when 18 months old (no resulting broken or fractured bones).
– Non-restorative sleep since age 7, when began waking up sluggish and with a tired-achy-pressure sensation around eyes. The sensation itself is present 24/7 and is still present today. (ENT doctors consistently report I have no sinus problems.) Tended to be constipated.
– Developed chronic gas at age 14
– Chronic fatigue since age 15, with gradual onset and no known infection that preceded the onset of fatigue
– At age 17 undertook an elimination diet and discovered refined sugars caused feeling ill, grains cause bloating, and cultured milk products make eyes burn. Since then I’ve loosely followed a paleo diet.
Earlier this year I tested positive for EBV antibodies, and I vaguely recall this was already true in my late teens, as well.
Recently I’ve tried Symbioflor-2 (concurrent with Symbioflor-1) for a week, and Act’Regen five days now, with no discernible reaction to either.
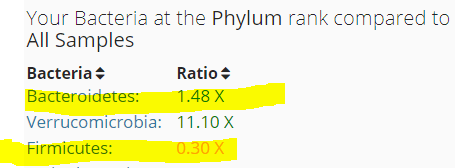
uBiome results
From the notes above, we have a much higher functioning CFS person than most. The uBiome results suggests that is the case — many items are much less severe than what is often seen in other’s uBiome.
Diversity 88%ile (Common on uBiome results for CFS)
 – E.Coli’s parent — much higher than most. But Genova Diagnostics lab report Zero for E.Coli specifically.
– E.Coli’s parent — much higher than most. But Genova Diagnostics lab report Zero for E.Coli specifically.
Bacteriodetes/Firmicutes shift is very moderate compare to other CFS patients

Sleep deprivation (possible Melatonin) families — not too bad, g low firmicutes; melatonin is not suggested
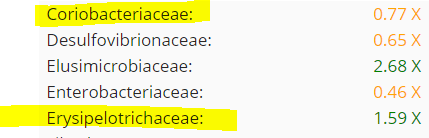
Proposed bacteria genus contributing to MCS: above threshold (0.32x)

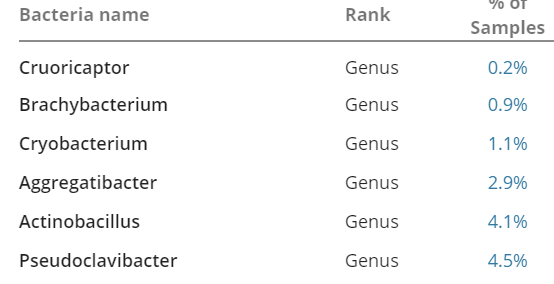
Uncommon Bacteria

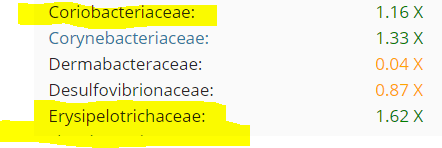
Overgrowths

Analysis of Overgrowth and Rare Genus
- Acholeplasmataceae (family)
- Alloprevotella (genus)
- Anaerotruncus (genus)
- Cronobacter (genus)
- Elusimicrobium (genus)
- Enterorhabdus (genus)
- Erysipelatoclostridium (genus)
- Oscillibacter (genus)
- Pseudobutyrivibrio (genus)
- Terrisporobacter (genus)
- Thalassospira (genus)
- Klebsiella pneumoniae (species) (From Genova Diagnostics)
NUTRIENTS/ SUBSTRATES
- L-Tryptophan – 3
- Iron supplements – 4, 12
- Acetoin – 4, 12
- “Acetoin is added to partially hydrogenated oils.” [Wikipedia]
- L-Lysine – 12
- Sucrose – 12
- L-Histidine -12
- D-Lactose -12
- Myo-inositol – 12
- Urea – 12
- D-Sorbitol – 12
- L-Ornithine – 12
- Iron supplements
- D-Lactose [parent]
- L-Rhamnose [parent]
INHIBITED BY
Walnuts -3- Gallate -3
- Gallate – 3
- Pomegranate ellagitannins – 4
- Flaxseed – 7, 8, 9
Cranberry bean flour – 10
ENHANCED BY
Cranberry bean flour – 2Walnuts -3, 8, 9- Saccharomyces boulardii – 3, 8, 9
- Berberine – 3
- Aspartame -3
- Partial Sleep Deprivation – 7 (connected to non-restorative sleep cited above)
- Resistant starch (type III) – 8
- Resistant starch (type II) – 8
- Resistant starch (type I) – 8
INHIBITS
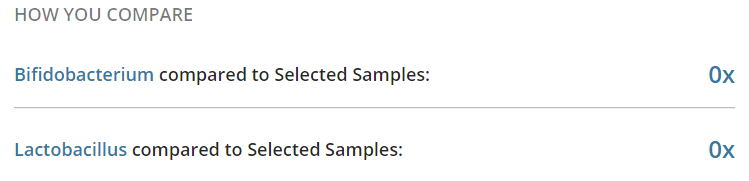
- Bifidobacterium 3, 4, 8, 9
Despite 11 genus listed, there is little known information on what makes them tick. Flaxseed porridge with a glass of Pomegranate juice for breakfast is the only clean suggestion.
Elusimicrobium is a new genus to me (a.k.a. Termite Group I), I have not seen it in other uBiomes. It is both rare and the greatest relative overgrowth. Going over to http://www.genome.jp/ we can discover what antibiotics it may be resistant to (based on it’s DNA):

Digging into PubMed, we find:
- ” an unusual peptide degradation pathway comprising transamination reactions and leading to the formation of alanine, which is excreted in substantial amounts. ” [2009]
- “The isolate grows heterotrophically on sugars and ferments D-galactose, D-glucose, D-fructose, D-glucosamine, and N-acetyl-D-glucosamine to acetate, ethanol, hydrogen, and alanine as major products but only if amino acids are present in the medium. ” [2009]
- “Unexpectedly, Elusimicrobia made up 14% of the operational taxonomic units detected in one subject at day 7, which is the only value that contributes to the Elusimicrobia average abundance of 3% for that date. This may be due to a subject that originated outside of North America with some rarely reported microbiome taxa.” [2017] – in this study, yogurt increased it’s abundance.
Avenues to Explore
These are based on history and labs that were included.
Epstein–Barr virus (EBV)
- Lactobacillus casei Shirota probiotic (Yakult) – “A similar effect was found for plasma EBV antibody titres in EBV seropositive participants (p < 0.01) with antibody titre falling in the probiotic group but increasing in the placebo group over time.” [2016]
Hypercoagulation
- See this post, it may account for cognitive, sleep and other issues.
IBS Probiotics
- See this post and the literature supporting these specific probiotics.
High Triglycerides, Cholesterol
We know that some bacteria increases it (and may be a contributing factor), so looking at those known to lower it (perhaps by taking out the other strains).
- Lactobacillus Fermentum reduces – so keep taking it
- Lactobacillus sp. JNU 8829, L. acidophilus KU41, L. acidophilus M23, L. fermentum NS2, L. plantarum M13, and L. plantarum NS3 were found to reduce cholesterol levels by >50% in vitro. ” [2015] Note these are specific strains from Korea.
- “Bifidobacterium animalis subsp. lactis BB-12..did not improve lipids, lipoproteins and total and individual fecal short chain fatty acids ” [2017] i.e. this one has no effect.
- “a commercial spore-based probiotic supplement [Bacillus indicus (HU36), Bacillus subtilis (HU58), Bacillus coagulans, and Bacillus licheniformis, and Bacillus clausii] for 30-d…. supplementation was associated with a 42% reduction in endotoxin and 24% reduction in triglyceride” [2017] See this post for commercial products.
- A review of old studies is here [2016]
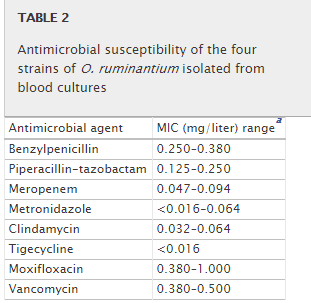
Antibiotics for Oscillibacter
The “grains cause bloating,” combined with Oscillibacter being enhanced for Resistant starch Type I, II, III hints that this may play a significant role.
There is a 2013 study from Denmark treating this genus, the antibiotics tested are shown below. Tigecycline is a tetracycline and metronidazole is a common antibiotics that generally reports good results with CFS patients.
Bottom Line
There was no clear clustering of nutrients or inhibitors in the rare or overgrowth. If iron supplements are being taken, consideration should be done for stopping them (see this post on the bacteria connection for iron, and “Could iron supplement makes CFS recovery harder?”
Given the food sensitivities reported, the reader will need to slowly feel out the best path.
As always, consult with your medical professional before adding probiotics, changing supplements etc.















 From
From