Updating my notes on Oregano today, I came across this study:
- “Results showed that protein, pH, aw, presence of beef extract, sodium lactate and nitrates did not influence their antimicrobial effect. In contrast, the presence of pork fat had a negative effect against both [Garlic and Oregano] Essential Oils [EO] associated with their dilution of the lipid content. The addition of food phosphates also exerts a negative effect against EOs ” [2017] A common source of pork fat are hot dogs and sausages.
- “[Potato] Starch and [sunflower] oils concentrations of 5% and 10% had a negative impact on the EO efficacy. On the contrary, the EOs were more effective at high concentrations of protein, and at pH 5, by comparison with pH 6 or 7. ” [2008]
- ” EOs retained greater efficacy at pH 5 and 2.32% sugar…moderate levels of simple sugars.” [2009]
And from prior posts dealing with food additives:
- ”geographical variation in Crohn’s Disease [CD] correlates with emulsifier consumption as does the increasing incidence of CD in Japan; … very small concentrations of the emulsifier polysorbate 80 enhance bacterial translocation across intestinal epithelia.” [2013] See this post for more and this one on Endocrine Disruptors.
- ”we determined that the polysaccharide dietary additive, maltodextrin (MDX), impairs cellular anti-bacterial responses and suppresses intestinal anti-microbial defense mechanisms”[2015]
- Avoid Emulsifers, (sometimes they are called “Conditioners” on labels) especially
- maltodextrin
- polysorbate 80
- carboxymethylcellulose[E466]
- Sodium stearoyl lactylate
- Calcium Stearoyl-2-Lactylate
- “Findings from epidemiology studies indicate that diets high in animal fat and low in fruits and vegetables are the most common pattern associated with an increased risk of IBD. Low levels of vitamin D also appear to be a risk factor for IBD. …. Unfortunately, omega 3 supplements have not been shown to decrease the risk of relapse in patients with Crohn’s disease. … Although fiber supplements have not been definitively shown to benefit patients with IBD, soluble fiber is the best way to generate short-chain fatty acids such as butyrate, which has anti-inflammatory effects. Addition of vitamin D and curcumin [Turmeric] has been shown to increase the efficacy of IBD therapy. There is compelling evidence from animal models that emulsifiers in processed foods increase risk for IBD.” [2016]
- “dietary emulsifiers interact with the multilayered endogenus mucus secretaions that coat the luminal surfaces of the intestinal tract and may compromise the ability of the human mucus to prevent contact between microorganisms and intestinal epithelial cells. Because emulsifiers have become ubiquitous ingredients in virtually all processed foods and beverages, including many that claim to be “organic”… [2016]
Bottom Line
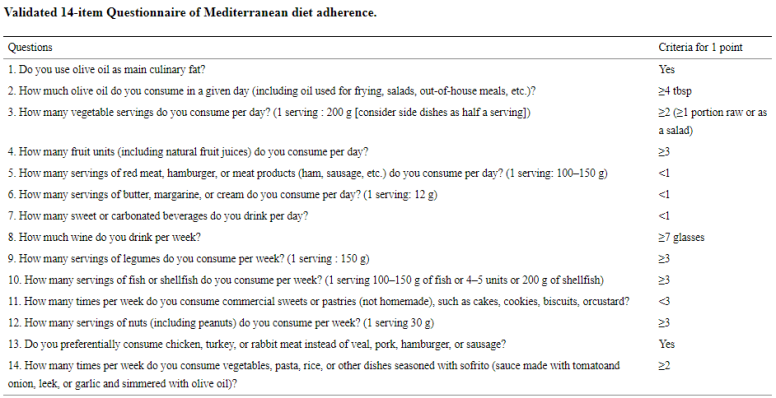
Processed food is likely a significant contributor to IBD/IBS/FM/CFS. Population study also associate non-Mediterranean diet pattern with higher incidence of IBD. Pork and using sunflower oil (use Olive oil instead) is likely a food to exclude from your diet if you are taking herbs or essential oils because they reduce the herbs effectiveness. Avoid foods that lists emulsifiers and phosphates. Keep a note on your smart phone of the name of the common emulsifiers listed above.
And Yes, “Virginia there are organic emulsifiers in organic food…. “ — avoid them. Organic does not mean unqualified safe or good.