This evening on NPR News, I saw their story on Long COVID and pending work. You may view the segment here. From watching ME/CFS research for several decades, “I wept” for Long COVID patients — I do not expect any of this planned work to produce relief to patients.
The video below are my feeling about what Long COVID is, how to approach detection and treatment.
Key Points
Like with another post-infection syndrome, Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), decades of research has failed to find a magical single key factor nor an effective new drug to treat.
Their core assumption is that there must a simple single factor
The reality is that there are dozens of factors with commonality across patients, they are also highly individual factors.
Studies have constantly shown microbiome dysbiosis as a signature. A large number are shifted. What is reported in studies can be reviewed here.
We can see this in contributed microbiome samples from people with Long COVID. You can see those shifts on this page.
There are clinical issues with this approach — because of a lack of standardization of microbiome tests used in studies and clinics. See this post. There are issues which can be resolved with some effort.
Looking at bacteria from different labs, we find almost no agreement. If we use KEGG data on samples from different labs, we end up with agreement on which metabolites are abnormal across different labs.
We have demonstrated the ability to accurately predict Long COVID from microbiome samples as shown by a patient agreement with the predicted symptoms illustrated below:
We are able to generate suggestions of probiotics, supplements, etc that will reduce the symptoms with a high success rate.
In the past, when I had active ME/CFS. I could describe it as a flare sufficient to put me on disability. I would sit on the computer playing a variety of simple puzzle games. AAs the flare eased and my cognition improved, I began to find those games boring and moved on to more mentally challenging puzzles.
Today, I am fully in remission, particularly from the cognitive issues often described as brain fog. Still, I make it a daily habit to complete two free logic problems on LinkedIn.
Zip
This is the simplest (almost boring). You need to find a path connecting all of the numbers in order and use every square.
LinkedIn provide additional games at https://www.linkedin.com/games/. You may need to create a FREE linkedin account to access them.
Bottom Line
I’ve found this routine valuable for several reasons:
It lets me compare my performance with other professionals. At 73 years old, I’m often competing against people half my age—and my times are usually better than their averages.
It serves as an excellent “wake-up activity” first thing in the morning.
It acts as a personal monitoring tool: if my performance starts to slip, it may be an early warning sign of relapse, reminding me that it’s time to rotate or adjust my probiotics.
27 years ago, I was diagnosed with ME/CFS. Even as far back as the early 1970s, while at university, I experienced severe cognitive difficulties—including a sudden decline from managing triple honors to simply trying to finish my degree. At the time, my physician correctly attributed these issues to stress, though the biological mechanism was unclear. Today, it’s recognized that stress can readily disrupt the microbiome, contributing to dysbiosis.
During these 27 years, I’ve thoroughly reviewed most of the scientific literature on ME/CFS. I was a subscriber to the Journal Of Chronic Fatigue Syndrome throughout its publication from 1995 to 2007. I’ve experienced multiple relapses, often triggered by stress, leading me to adopt a preventative approach: avoid stress when possible. My guiding philosophy now is “Que Sera, Sera (Whatever Will Be, Will Be)”—which can be especially challenging given the current political climate in the US.
ME/CFS and Long COVID (LC) are both highly heterogeneous, varying widely in symptoms and duration; specific symptoms of LC can change or resolve unpredictably over time. Studies—including those involving twins and across genders—demonstrate that such diversity complicates the search for a universal treatment that provides consistent symptomatic relief.
My Criteria
Recently, friends have sent me several new studies asking for my feedback. Given years of seeing the field marked by repeated announcements of “breakthroughs,” my essential question remains:
“Do these papers suggest immediate, actionable clinical steps? “
“Is there robust evidence that these interventions benefit a substantial proportion of people with ME/CFS?”
To see if the papers do not met those criteria, I will quickly review them. I will neither get hopes up nor excited about them if they fail…. they are speculation. Speculation is awesome for getting grants for research but not for improving patients. Getting excited about them and the subsequent disappointment is not healthy for the microbiome.
Treatments primarily involved rotating courses of appropriate antibiotics and administering suitable anticoagulants. Both methods can profoundly affect the microbiome; for example, anticoagulation improves oxygen levels, creating conditions that affect bacterial growth patterns. My guiding principle—KISS (Keep It Simple, Stupid)—leads me to focus on the belief that the underlying issue is persistent microbiome dysbiosis.
This conviction is why I dedicated substantial time and some personal resources to the development of the free Microbiome Prescription website, which was originally designed with a sole focus on ME/CFS.
Being a former University Instructor at Chapman University for Artificial Intelligence, my first item was check cross validations. “including ‘omics altogether (AUC=82.3%), immune (78.5%), KEGG (69.1%), species (71.5%), and metabolome (76.4%), while Glmnet excelled in Quest data (74.8%)“. The study did use Shotgun sampling but ignored The taxonomy nightmare before Christmas… (the blue whale in the room).
Key Bottom line — There was no treatment suggestions or protocols
A ton of issues were identified …. ” This map uncovers disrupted associations between microbial metabolism (e.g., short-chain fatty acids, branched-chain amino acids, tryptophan, benzoate), plasma lipids and bile acids, and heightened inflammatory responses in mucosal and inflammatory T cell subsets (MAIT, γδT) secreting IFNγ and GzA.” but no discussion of a unified treatment for all of them. ME/CFS is complex.
My own approach, the microbiome dysbiosis, is very treatable as demonstrated by Microbiome Prescription, some examples of treatment suggestions are here. Since it is likely that the microbiome drives most of the above issues — life is simpler and improvement can happen in weeks in many cases. All of the issues cited in this paper, listed below, has evidence that the microbiome is a significant contributor.
ME/CFS is characterized by persistent fatigue, post-exertional malaise, multi-site pain, sleep disturbances, orthostatic intolerance, cognitive impairment, gastrointestinal symptoms, and other issues. This complexity not only hinders timely diagnosis but also poses significant challenges for effective treatment.1,2,3. The pathogenesis of ME/CFS is not well understood, with some triggers believed to include viral infections such as Epstein-Barr Virus (EBV)4, enteroviruses5 and SARS coronavirus6, in addition to bacterial infections and other causes7.
My conclusion is simple, it is a viable candidate for treatment…. BUT….
The BUT with Single Item Treatments!
If the root issue is microbiome dysbiosis, no single item is likely to be sufficient to be a “magic cure all”. We are not talking about eliminating a single virus or bacteria. A single virus or bacteria belief has been rampant with ME/CFS researchers for decades. Why? Simple, treating a dozen shifts at the same time is too complex given the methods available. But it is not too complex with a suitable fuzzy logic expert system running of several million facts.
On the last article the reader wrote:
I find it interesting because they found the correlation with the microbiome. I wonder why researchers don’t look more at it.
The reason is simple – they lack the skills and training to deal with it. Additionally, there is the absence of data in a suitable form. IMHO what is needed?
Training in the full range of Artificial Intelligence methods. I have found fuzzy logic is essential. It is rarely taught in AI classes today, everything has shifted to the hottest tech: Large Language Models (LLM, ChatGPT) that is well known for hallucinations.
A suitable database, a summary of the data used for the fuzzy logic engine is here. Some analysis uses over 13 million facts encoded into a database. Most of these facts would not “be seen” using the bots that provides data to LLM due to paywalls and other factors.
Suggested reading (intro book with a sample of the text)
In the first post of this series, Probiotics Fundamentals: Part 1 Specific Strains I cited strains that are available retail that has been researched. The logical starting point is to search for your needs, read the studies and then rank the probiotics in prefer order for doing a personal trial. You want to do one probiotic at a time with rotation and described in the prior post (see prior post).
To searching for strain specific studies of probiotics available retail. Click here.
No Study found or issue not listed
The next step is to look at the conditions that I have abstracted/extracted studies for, listed at “U.S. Nat. Lib. Medical Conditions Studies with Microbiome Shifts“. We are shifting from strain to species level. This gives several paths, let us examine Autism. There are
Based on Publish Studies of Species
Clicking on [Can You Help Improve Suggestions] will take you to a page. At the bottom you will see “Treatment Substances” which lists things that have helped in studies. Scan it for probiotic names, for example:
Which suggests L. Reuteri with inulin may help. The source is linked. Make sure you read them.
Based on Deficiencies of Probiotic Bacteria
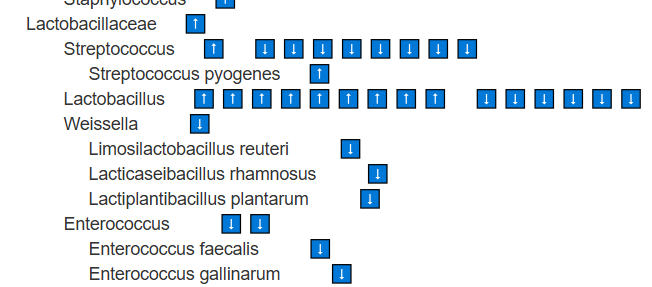
Clicking on Taxons will take you to a page showing all of the bacteria shifts reported for the condition.
Look for Lactobacillus, Bifidobacterium,etc with
These species are found at lower levels, suggesting their metabolites are also reduced. Supplementing with them as single-strain probiotics is logical. Stay at the species level (e.g., Bifidobacterium longum) rather than higher classifications such as the genus Bifidobacterium. In general, avoid probiotic mixtures, as they may include strains that are counter-indicated (e.g., Bifidobacterium catenulatum, Bifidobacterium breve) or strains for which we lack sufficient information.
Based on Modelled correction of Bacteria
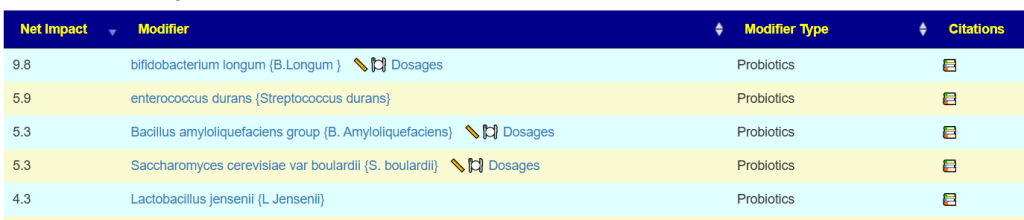
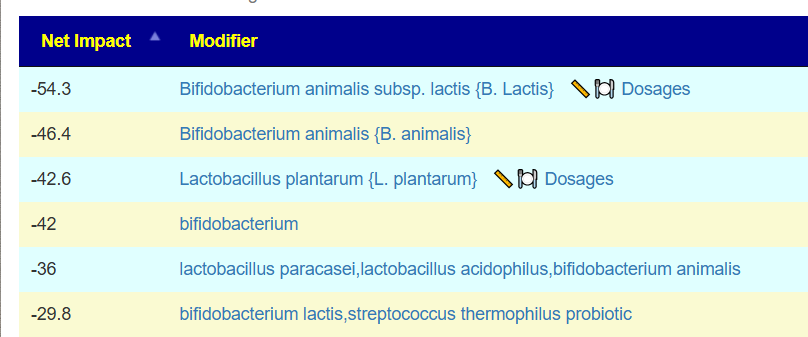
Clicking on Candidates, will send the huge bacteria list above through a fuzzy logic expert system to compute suggestions with weights given for each one.
The issue comes from the fact that the model/studies is based on multiple subgroups of people with Autism (or other conditions). The data might be accurate within each subgroup, but when you merge them together, you can end up with contradictions. So it’s not really a problem with the approach—it’s a problem with the data mix.
The best rule of thumb is to start with the things that show up as agreements across the data. For example: Bifidobacterium longum and Limosilactobacillus reuteri. Once you’ve tried probiotics that have clear agreements, then you can carefully experiment with the ones where there’s disagreement and see how your body responds.
The next level up in Probiotic Suggestions
It is pretty simple, get a microbiome test. My preferred tests are:
Thorne for shotgun (more expensive but much higher detail)
You want to ideally get a test that reports on all of the common probiotic bacteria. Many common tests do not report many of these. For example: Diagnostic Solution GI-Map reports only
On the other hand both of the above tests report species.
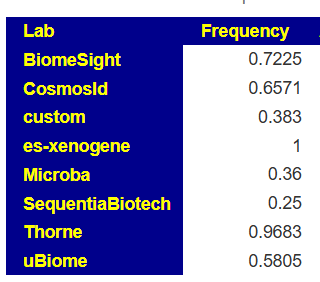
When you select a test, you should check Microbiome Prescription to see what the detection rate is. For example for Bifidobacterium longum, we see how often this is detected in samples.
For the shotgun tests (Xenogene and Thorne) we see 96% and 100% of the time, if it show low, you can have confidence in taking some
For SequentiaBiotech we see it is seen 25% of the time. If you have none reported we are left being uncertain if you actually have none or is the none because of the test’s methodology
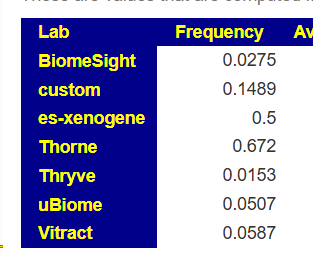
Another example is L.Reuteri where the shotgun tests find in in over 50% of samples, while some 16s finds in only 2% of samples.
Bottom Line
We’re piecing things together from lots of scattered knowledge, and there’s no single standard method—either for testing microbiomes in labs or for the studies themselves. Nothing here is clear-cut; everything’s kind of fuzzy, sometimes super fuzzy. In this post, the focus was on picking probiotics for a condition using literature (an “a priori” approach). Basically, it means trusting the data at face value, even though we know it isn’t rock-solid.
This post started listing to a Pod Cast from The Economist. I am not sure if the pod cast and article is available to non-subscribers so I will do a few quotes from it:
Creatine works mainly by increasing the amount of energy that muscles can produce. Cells use a molecule called adenosine triphosphate (ATP) as a carrier of chemical energy. Aerobic respiration, which uses oxygen to break down fats or sugar, is by far the most efficient way of making ATP. But it is relatively slow. When muscles need a lot of ATP in a hurry most of it is supplied instead by the phosphocreatine system which, as its name suggests, relies on creatine to work.
As summarised in a review published in 2021 in Nutrients, some studies have suggested that creatine might sharpen things like short-term memory or reaction times. Others have reported it may lessen the symptoms of mental-health problems such as depression, and tentative evidence suggests it improves cognition in those with Alzheimer’s disease. Both may be associated with a misallocation of energy within the brain.
More Literature
Creatine (C4H9N3O2) is a ubiquitous molecule synthesized predominantly in the liver, kidneys, and pancreas at a rate of ~1 g/day via an interorgan process. [2024]. It is often low in people with ME/CFS; see MEPedia for more information.
Creatine and post-viral fatigue syndrome: an update [2025] “Emerging evidence highlights the role of mitochondrial dysfunction and creatine metabolism in PVFS, positioning creatine as a promising therapeutic candidate. While initial studies suggest its efficacy in alleviating fatigue and improving bioenergetics, further large-scale, rigorous trials are essential.”
Creatine monohydrate supplementation for older adults and clinical populations [2025] “when combined with exercise training, is safe and has beneficial effects on measures of whole-body lean body mass, regional muscle size, muscle strength, bone area and thickness, functional ability, glucose kinetics, cognition and memory.” “have application for treating age-related sarcopenia, osteoporosis, frailty, and those with metabolic and neuromuscular disorders.”
Going to iherb.com, we see one kilo is $21 on subscription. This is 200 dosages of 5mg (i.e. 10 cents a day). Some sources suggests 4 5mg dosages per day — so we have 2 months for $21.00. You can spend a lot more buying from fancy sources in capsules. I am a frugal person….
By some on a 6 month subscription. Cancel if it has no positive impact.
Gut Impact
For those interested, you can see what it changes on Microbiome Prescription. Of note is that it increases:
Children with autism reliably show lower ATP levels compared to neurotypical controls. [2011]
Impaired energy metabolism—including reduced ATP and other high-energy metabolites—correlates with features like poor methylation, low sulfate recycling, and high oxidative stress in autism.[2016]
Several studies report mitochondrial dysfunction in ASD, with deficits identified in electron transport chain activity and energy production, leading to abnormal ATP levels in brain and peripheral samples.[2011]
Some preliminary research and clinical trials are investigating creatine supplementation for ASD, focusing on cases with low brain creatine or known metabolic defects. [2025]
Bottom Line
It is cheap, safe and has significant potential benefits for many.