
A reader asked if this might be suitable with my model. Information was sparse but a 2010 studies suggests that the harm aspect may be greater than the good.
Low dose naltrexone: side effects and efficacy in gastrointestinal disorders. [2010] [Full Text]
- 58 of 121 had one or more neurological complaints – almost 50%
- In 13 patients with idiopathic irritable bowel syndrome, 2 were markedly worse.
- . In 85 patients with irritable bowel syndrome-small intestinal bacterial overgrowth, 15 were markedly improved, 32 were moderately improved, 11 were mildly improved, 23 were unchanged, 3 were moderately worse, and 1 was markedly worse. – Odds of getting better instead of worst is 14.5:1 .
As a treatment, yes — some improves, many have no change, and more became worst than better. This does not seem like a rational choice – it’s playing craps with loaded dice.
It has been studies in terms or Crohn’s Disease, a more severe disruption of the microbiome, “Currently, there is insufficient evidence to allow any firm conclusions regarding the efficacy and safety of LDN used to treat patients with active Crohn’s disease… is not without potential for side effects. Future use of methylnaltrexone may be better tolerated since it does not cross the blood brain barrier. ” [2014]
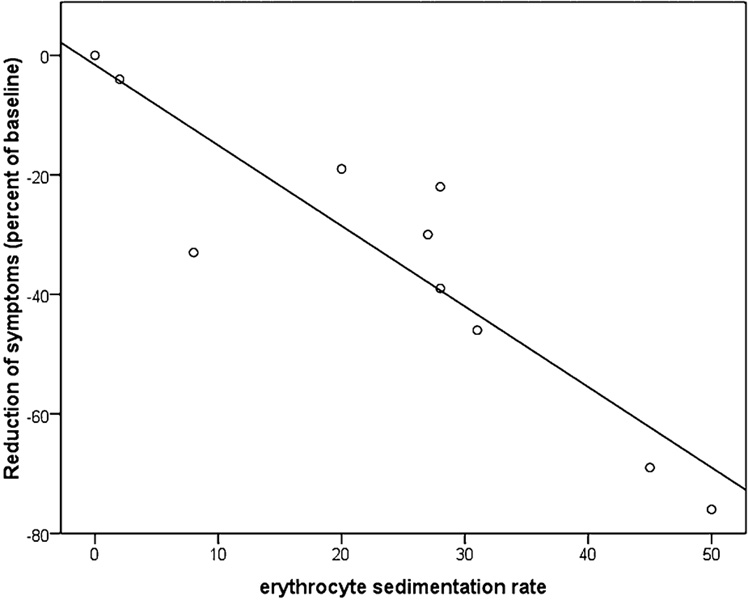
In terms of Fibromyalgia (FM) [2013], it appears to help — remember that FM is likely due to DNA factors — which suggest that its impact may be connected to this. Before taking it, your baseline erythrocyte sedimentation rate[ESR] should be taken to see if you are likely to be a responder, see table below.[2009]. Also, the effect decline within a week once you stop.
Like milnacipran, a related drug (which some suggest is better for FM), adverse effects can happen in 20-30% of patients [2009] “. “milnacipran 100 mg or 200 mg is effective for a minority in the treatment of pain due to fibromyalgia, providing moderate levels of pain relief (at least 30%) to about 40% of participants, compared with about 30% with placebo.” [2015] So only 10% improved more than those with a placebo…
There is no clear pattern of ESR for IBS[2015], FM [2016]. It appears to apply to a subset only (likely DNA associated) which can be determined from the ESR. With CFS, browsing web pages you will find normal ESR is reported by some and low by others. One subset has low SED rates (hence LDN will likely have no positive effect for them)
- According to Dave Berg, Hemex (hypercoagulation theory):
“The ESR (erythrocyte sedimentation rate – red blood cell sed rate) is called SED RATE for short. We are close to having enough data to publish that the normal range for SED RATES should start above 3 or 4. Values below this are correlated with high SFM values. As the Soluble Fibrin Monomer (SFM) goes up in the plasma, these molecules form dimers (2 stuck together). This physically blocks the RBCs from settling out of the plasma, thus a low sed rate.” [Townhall] – this is just ONE of the coagulation defects that he found in CFS. So some will be low and some normal and some high… - This happens to be true for me with non-prescription items effective to lower SFM.
This leads to the possible mechanism of action, it’s does impact one form of anticoagulant!! There are many forms of coagulation. Coagulation reduces oxygen level to tissue, and this is well recognized as a major source of pain – cells screaming for oxygen.
- “The fibrinogen levels declined sharply with abstention and an additive effect was noted with the administration of naltrexone,” [1994]
Bottom Line
There is no clear evidence of it being effective with microbiome disruptions. Yes, a small percentage of patients improved (which many MD’s see emotionally and then start prescribing it to all of their CFS patients). Many CFS MDs may discount or ignore the patients that became worst (unfortunately) because they are focused on positive results instead of evaluation of this drug. With a non-fatal disease, a physician tossing a drug that is more likely to worsen a patient than improve the patient raises some fundamental ethical questions.
If you have taken LDN and improved, don’t take exception with this post — I agree that you improved, the studies say that. You are the lucky ones…. others are not the same.
As a side note during my research I found “” With the exception of weak nonspecific DNA damage observed in an E. coli DNA repair test and possibly with WI-38 cells as well, Naltrexone did not demonstrate significant potential for the induction of gene mutations or chromosomal aberrations under the conditions of this evaluation.” indicating that there may be some long term risks. Damage to your microbiome DNA and your own DNA.
