In my last post, we saw that Niacin levels in the blood was often low with microbiome dysfunction. This trigger a memory of early in my second relapse taking the expensive NADH supplement because a study finding that it helped CFS.
NADH Studies
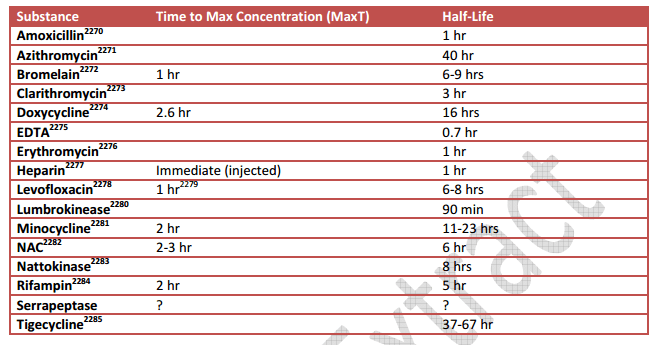
- Chronic lactic acidosis in an adult. A new syndrome associated with an altered redox state of certain NAD–NADH coupled reactions[1970].
- Therapeutic effects of oral NADH on the symptoms of patients with chronic fatigue syndrome[1999]. “The twelve patients who received NADH had a dramatic and statistically significant reduction of the mean symptom score in the first trimester (p < 0.001). However, symptom scores in the subsequent trimesters of therapy were similar in both treatment groups.” – short term effect only
- Is NADH effective in the treatment of chronic fatigue syndrome?[2000]
- Comparison of oral nicotinamide adenine dinucleotide (NADH) versus conventional therapy forchronic fatigue syndrome [2004].
- [Nicotinamide adenine dinucleotide (NADH) in patients with chronic fatigue syndrome] [2010].
Once I found that it was a precursor to niacin, I switched to taking much cheaper (flushing) niacin. It actually worked better!!! Turning lobster red and itchy skin is another matter!
Forms of Niacin
“Niacin and niacinamide are both forms of vitamin B-3, and they can be used interchangeably in daily doses of 100 mg or less. However, each form has specific health applications when used in higher doses. Niacin is often taken to support cholesterol levels already within the healthy range (both LDL and HDL), while niacinamide is used to help promote a healthy insulin response, as well as to help maintain joint health. A third form of vitamin B-3 known as inositol hexaniacinate is similar to niacin, but it does not produce the red, prickly flush that often accompanies the latter form, and for this reason it is commonly referred to as flush free niacin.” Swanson Vitamins
- “niacin can cause flushing and niacinamide probably cause thrombocytopenia.” [2014]
- “Nicotinamide supplementation induces detrimental metabolic and epigenetic changes in developing rats[2013]. “long-term high nicotinamide intake (e.g. induced by niacin fortification) may be a risk factor for methylation- and insulin resistance-related metabolic abnormalities.”
From Niacin: chemical forms, bioavailability, and health effects[2012]. the following was found interesting:
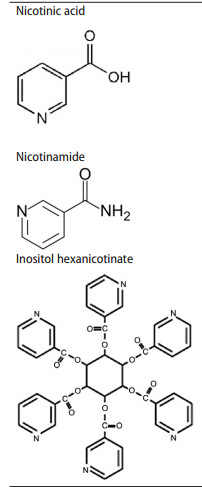
- NA – flushing niacin, aka. Nicotinic acid
- ER-NA – extended release nicotinic acid
- IHN – Inositol hexanicotinate
- NM – Nicotinamide (a.k.a. niacinamide, nicotinic amide)
“Clearly, NA is a very effective and inexpensive agent for improving health outcomes in persons with elevated lipid levels at risk for heart disease, but its utility is limited by poor patient compliance due to the generally unacceptable flushing reaction”
“There is debate about whether the bioavailability of NA from IHN is high enough to justify it being considered a form of niacin. Some publications support this classification, while others contradict it… data on the efficacy of IHN for lowering serum lipids do not support the hypothesis that the chemical forms are clinically interchangeable”
“Higher doses of NM have been tested for a variety of possible benefits related to several disease conditions such as depression,55 but results are inconsistent and NM is not generally recognized as an effective treatment for clinical depression or high plasma triglyceride and cholesterol levels”
“The data for a direct quantitative comparison of the ER-NA and NA forms are not robust, but the risk of hepatotoxicity seems approximately twice as high with the ER-NA forms compared with the crystalline NA form.”
“This analysis indicates that, contrary to the common and mistaken perception, the four major forms of niacin in the marketplace (NA, ER-NA, IHN, and NM) are not bioequivalent with respect to efficacy or safety.”
What is a flush?
“High intakes of NA(Niacin) produce a vasodilative effect that can result in an intense itching or burning sensation of the skin known as the “niacin flush.” Flushing may be classified as a nuisance effect. It is initiated via prostaglandin D2-mediated vasodilatation of small subcutaneous blood vessels. The vasodilatation is associated with an unpleasant sensation of intense warmth and itching that commonly starts in the face and neck and can proceed down through the body. Some individuals may experience a rash, hypotension, and/or dizziness. Flushing appears about 30 minutes after intake of NA, and 2–4 hours after intake of ER-NA. Skin-flushing reactions usually persist over only a few doses until the body develops a natural tolerance. The daily dose is generally administered over several hours in three parts to reduce flushing.
Although flushing is a common side effect with both the free nicotinic acid and the extended-release forms, it is possible to ameliorate this symptom by ingesting niacin with food, avoiding alcohol, and, for those individuals on aspirin therapy, consuming aspirin one-half hour before ingesting niacin. The free nicotinic acid form can be taken with multiple meals in divided doses, making it possible to achieve therapeutic goals.”
Bottom Line
They are not the same. I prefer NA – classic niacin. The flush usually clear out my brain (when it happens). Usually I do not get a flush, but when I do it is suggestive that something is changing in my system — perhaps increased growth of bacteria producing toxins.
While there is a total absence of studies dealing with Niacin and Chronic Fatigue Syndrome, Irritable bowel disease, Fibromyalgia, it has been found to be low in the blood of other microbiome dysfunction. It is part of natural vascular dilation which suggests a low level may result in tighter blood vessels and less oxygen delivery (more brain fog). From personal experience, I recommend it.