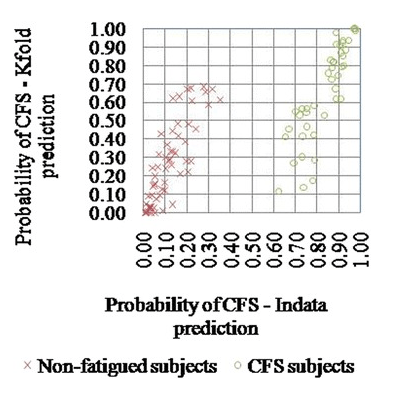
Another DNA study was published in Oct, 2015 out of Norway which appears to be included in 23 and me results, but the key SNP is not there. It looked at the SLC6A4 gene. This gene is associated with OCD and anxiety (which could present before CFS). An earlier 2015 study from Finland/India demonstrated that examining multiple SNPs at the same time was reasonable good in predicting people with CFS when some 1-200 SNPs were considered in combination. The study size was way to small to be used in practice.
Looking up on 23AndMe
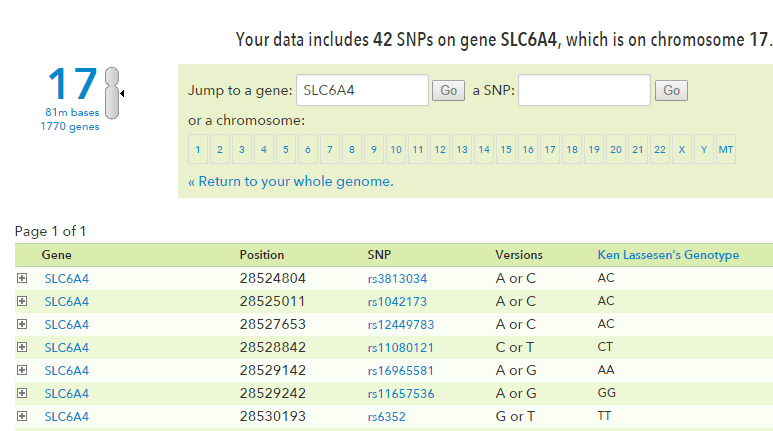
After you logon to 23andMe, click the link below
https://www.23andme.com/you/explorer/gene/?gene_name=SLC6A4
And this should appear:
“Patients with the SS or SLGgenotype had a significantly lower number of steps per day and also a significantly higher FDI score than patients with the LALG, SLA or LALA genotype when gender was taken into account as a covariate… we found that CFS patients with the 5-HTT SS or SLG genotype had a more pronounced reduction in physical and psychosocial functioning than patients with the 5-HTT LALG, SLA or LALA genotype. This suggests that patients with the 5-HTT SS or SLG genotype have a less favorable 30 weeks outcome than patients with the 5-HTT LALG, SLA or LALA genotype.”
FYI: The LALG, SLA or LALA genotype are associated with medium to high serotonin production [2013].
” In accordance with previous studies of Caucasians or European Americans indicating a general 5-HTT SS or SLG genotype frequency of about 25% [6,10], the same genotype frequency was 26% in the patients and 21% in the controls. Thus, the 5-HTT genotype cannot explain why some individuals develop CFS.” – IMHO, it is associated with how the body responds to the microbiome shift seen in CFS.
Details
This link should take you directly to the SNP cited (SNP rs25531 A > G),
https://www.23andme.com/you/explorer/snp/?snp_name=rs25531
| (A;A) | 2.5 | short form of 5-HTTLPR. lower levels of serotonin, slightly less happy, benefits from more support |
| (G;G) | 2.1 | long form of 5-HTTLPR. less sensitive to pain |
It is in the 23andme DNA(Thank you Livewello.com for catching the typo!) —

On Health Rising, it has been reported as “unreliable” My personality type is a Polly-Anna, which would be consistent with the Genotype.
Recent related Studies
- Gene-Environment Interaction in Youth Depression: Replication of the 5-HTTLPR Moderation in a Diverse Setting.Rocha TB, et al. Am J Psychiatry, 2015 Oct. PMID 26315979
- [Association between the 5-HTTLPR Polymorphism of Serotonin Transporter Gene and EEG in Young and Postmenopausal Women].VolF NV, et al. Zh Vyssh Nerv Deiat Im I P Pavlova, 2015 May-Jun. PMID 26281230
- Regional brain disorders of serotonin neurotransmission are associated with functional dyspepsia.Tominaga K, et al. Life Sci, 2015 Sep 15. PMID 26232557
- Substrate and Inhibitor-Specific Conformational Changes in the Human Serotonin Transporter Revealed by Voltage-Clamp Fluorometry.Söderhielm PC, et al. Mol Pharmacol, 2015 Oct. PMID 26174773
- Serotonin Synthesis and Reuptake in Social Anxiety Disorder: A Positron Emission Tomography Study.Frick A, et al. JAMA Psychiatry, 2015 Aug. PMID 26083190
Bottom Line
We cannot use 23andMe results to check our status — however, if prior to CFS, you were prone to OCD or Anxiety, then it is more probable that you have this gene variation.
For 25% of CFS patients, serotonin supplementation my result in improved results (especially with those with OCD or Anxiety prior to CFS).