A reader who has several family members with conditions that have microbiome shifts associated asked about cardiac disease, which is frequent in one side of the family.
Below is what I could find. This is a new area of research that I expect to explode in the next few years.
” Dysbiosis of the intestinal flora has been associated with insulin resistance, diabetes mellitus and cardiovascular diseases, such as atherosclerosis and heart failure. ” [2019]
” In the recent years, both human and animal experiments have revealed that alterations in the composition and function of intestinal flora, recognized as gut microflora dysbiosis, can accelerate the progression of cardiovascular diseases. “[2019]

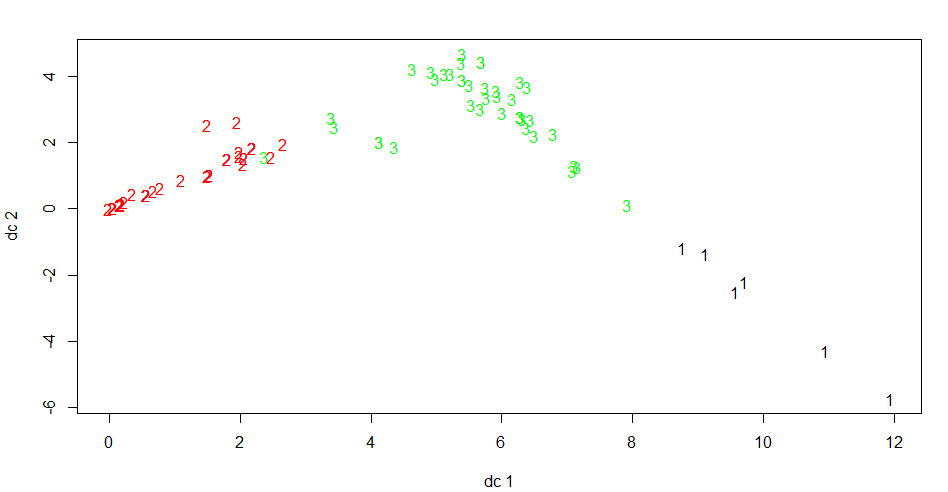
The gut microbiomes of VC and CAD patients were significantly different in terms of beta-diversity. Bacteria from Veillonella dispar, Bacteroides plebeius and Fusobacterium were enriched in the VC group, while members of Collinsella aerofaciens, Megamonas, Enterococcus, Megasphaera, Dorea and Blautia were decreased. According to the association with dyslipidemia, seven operational taxonomic units (OTUs), including Parabacteroides distasonis, Megamonas, Fusobacterium, Bacteroides sp., Bacteroides plebeius, Lactobacillus and Prevotella copri, were regarded as potential pathogens for CVDs. Additionally, Prevotella copri might be a keystone of CVDs, especially in VC patients, while Collinsella aerofaciens is a possible keystone of CAD, based on the multi-correlations of these bacteria with other OTUs in microbial communities.
The intestinal microbiota associated with cardiac valve calcification differs from that of coronary artery disease[2018].
- Suppression of the gut microbiome ameliorates age-related arterial dysfunction and oxidative stress in mice.[2019]
- Higher Fecal Short-Chain Fatty Acid Levels Are Associated with Gut Microbiome Dysbiosis, Obesity, Hypertension and Cardiometabolic Disease Risk Factors. [2018]
- Loss of Gut Microbiota Alters Immune System Composition and Cripples Postinfarction CardiacRepair. [2019]
- The gut microbiome and heart failure. [2019]
- Interaction between gut microbiome and cardiovascular disease. [2018]
- Design of the GutHeart-targeting gut microbiota to treat heart failure-trial: a Phase II, randomized clinical trial. [2018]
Bottom Line
You will note that almost all of the studies cited above were done this year and last year. This is an area that is actively being researched because the evidence indicate strongly that there is a relationship.

Because cardiac disease has many divisions and the amount published on each is sparse, I will not include this on my analysis site yet.