A reader asked me to do a review of Spectrumceuticals Pro4-50 D-Lactate Free Probiotics which contains
- L. rhamnosus,
- B. lactis,
- B. breve and
- B. longum.
Custom Probiotics offers a similar one labeled with the strains.
- L. Rhamnosus, Strain LR-32
- L. Salivarius, Strain LS-33
- B. Lactis, Strain BL-04
- B. Bifidum, Strain Bb-06
- B. Infantis, Strain Bi-26
- B. Longum, Strain BL-05
The latest incursions into the probiotic market of claims have posited the amelioration of oxidative stress via potent antioxidant attributes or limiting the administration of probiotics to those species that do not produce D-Lactic acid (i.e., claims that D-Lactic acid acidosis is linked to chronic health conditions)..there is no place in science and medicine that supports unsubstantiated claims. Extravagant industry based notions continue to fuel the imprimatur of distrust and skepticism that is leveled by scientists and clinicians at an industry that is already rife with scientific and medical distrust and questionable views on probiotics.
Probiotics, D-Lactic acidosis, oxidative stress and strain specificity [2017]
We should note a few things from the literature:
- ” Gut permeability markers (D-lactate and diamine oxidase (DAO)) …. the serum DAO activity and D-lactate concentration significantly increased by fluoride” [2020]
- Translation: No fluoride toothpaste or fluoridated water (beware of bottled water – it’s often sourced from civil fluoridated water systems)
- “The indicators of intestinal mucosal barrier function, such as D–lactate, endotoxin, and diamine oxidase, were significantly improved and the systemic inflammation (interleukin 10) was attenuated after probiotic [live Clostridium butyricum plus Bifidobacterium infantis] therapy. “
- “D-lactic acidosis is characterized by brain fogginess (BF) and elevated D-lactate and occurs in short bowel syndrome…. SIBO was more prevalent in BF than non-BF group. After discontinuation of probiotics and a course of antibiotics, BF resolved and gastrointestinal symptoms improved significantly (p = 0.005) in 23/30 (77%).” [2018]
- “Compared with control, d-lactate content, diamine oxidase activity, and adrenocorticotropic hormone level in serum decreased significantly [with Bacillus licheniformis]” [2013]
- “a stand-alone synbiotic treatment was started, specifically Bifidobacterium breve Yakult and Lactobacillus casei Shirota as probiotics, and galacto-oligosaccharide as a prebiotic. Serum D-lactate levels declined, and the patient has been recurrence-free for 3 years without dietary restriction.’ [2013]
- ” she was treated with sodium bicarbonate and oral antibiotics. The probiotics the patient had taken were likely the cause of D-lactic acidosis and should therefore be avoided in patients with short bowel syndrome.” [2009]
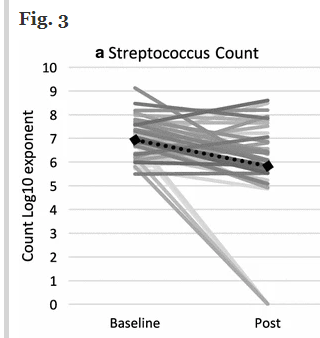
The reader requesting this review cited “Open-label pilot for treatment targeting gut dysbiosis in myalgic encephalomyelitis/chronic fatigue syndrome: neuropsychological symptoms and sex comparisons’ 2018. Which used the above mixture. “A small, negative correlation was observed between change in D:L lactate concentration ratios and change in Streptococcus count for the total sample (r s = − .243, p = .142). ” This is NOT STATISTICALLY SIGNIFICANT ( p < 0.01 is what we want to see). In fact, a chart in it illustrated the problem of using averages with the microbiome.
Bottom Line
The apparent reason for the promotion of D-Lactate Free probiotics is to reduce D-Lactate levels. There is no gold standard (or even silver standard) evidence that the above probiotics will do that. The dominant successful way of treating D-Lactic Acidosis is with antibiotics and avoidance of probiotics.
The best documented, all probiotic treatment is:
- Clostridium butyricum plus Bifidobacterium infantis
Promoter’s Moral Obligation
IMHO, the promoter of these products is under a moral obligation to demonstrate with a study that they work. For these products, a study with 15 control and 15 with brain fog/high d-lactate by lab, is a very very low cost study. Take DAO and D-Lactate readings at start for all, give them the probiotics for 30-90 days, remeasure… then publish. BEAUTIFUL MARKETING MATERIAL. The absence of such publications strongly suggests that this is now pure marketing hype (based on a logical idea and being “sold” on logic and not on evidence based studies). A study likely was done with no (or negative) results – which is exactly what was reported in the above study [that did get published, likely because it was a registered trial].
The Dilemma
The literature indicate that reducing D-Lactate also reduces DAO. Insufficient DAO is associated with Mast-Cell Activation and Histamine issues. There is a need for a balance here. A tightrope that may need to be carefully walked.
Sleep Consequences
Sleep issues in ME/CFS may be connected to excessive D-Lactic acid (A known characteristic of ME/CFS)
Results and conclusion: Administration of L-lactate does not influence sleep-wake cycle of experimental animals. At the same time, its artificial optical analog D-lactate induces the significant (as compared to the control) decrease in wake (34.8% to 26.5%) and increase in slow wave sleep (57.4% to 69.2%). It has been suggested that D-lactate may be the antagonist of one or several L-lactate receptors.
[D-lactate as a novel somnogenic factor?] [2020]