“transplantation of a healthy microbiota [FMT] is associated with reduced pain and improved quality of life. ” This option is rarely available since FMT is only authorized for recurrent Clostridioides difficile infections
And “Since mice transplanted with the FM gut microbiota showed reduced levels of specific bile acids (e.g., ursocholate) and bile-acid-metabolizing bacteria (Lachnoclostridium scindens [sic: Clostridium scindens] ), we treated mice that received FM FMT with UDCA, a host-derived primary bile acid metabolized in the mouse gut into various secondary bile acids.57,58,59 “
This post is running from this data into a model and thus a theoretical protocol (not tried in any clinic) if there is evidence to support a model.
Ursocholate Deficiency
This is available as a prescription drug: Actigall, Urso 250, Urso Forte. More details from WebMD. This is not always possible to get prescribed. This leads us to look for production by bacteria. We find that we have information about it on the KEGG: Kyoto Encyclopedia of Genes and Genomes. Going though databases, we do not find any known bacteria (including probiotics) that produces it 😦 . Going to a secondary data resource we get some bacteria involved in production:
Bottom Line — No evidence confirming the proposed mechanism
Science is endless iteration of tossing out hypothesis and then testing them. Revising as needed. In the study, it is probable that FMT does help; the speculation as to the cause appears unsupported and suspect.
1. Epstein-Barr Virus (EBV) EBV, which causes infectious mononucleosis, is one of the most frequently implicated viruses in ME/CFS. Studies show that 8–15% of people who develop infectious mononucleosis go on to meet ME/CFS criteria, and a subgroup of ME/CFS patients show evidence of EBV reactivation or immune response abnormalities related to EBV5 7.
2. Human Herpesvirus 6 (HHV-6) Reactivation of HHV-6, another common herpesvirus, has been hypothesized to contribute to ME/CFS symptoms, particularly in combination with EBV reactivation7.
3. Enteroviruses Historical and contemporary evidence links enteroviruses (a group that includes polioviruses, coxsackieviruses, and echoviruses) to ME/CFS. Outbreaks of ME/CFS have coincided with enteroviral epidemics, and some researchers consider enteroviruses a likely culprit, especially in cluster cases1.
4. Influenza Viruses Influenza infection has been associated with a more than two-fold increased risk of developing ME/CFS in the years following infection17.
5. SARS-CoV-2 (COVID-19) Many individuals with long COVID meet criteria for ME/CFS, and SARS-CoV-2 is recognized as a trigger for ME/CFS in some cases67.
6. Other Herpesviruses Varicella zoster virus (which causes chickenpox and shingles) and other herpesviruses have also been reported as potential triggers7.
7. Ross River Virus This mosquito-borne virus has been linked to ME/CFS onset, likely through immune system dysregulation3.
8. Retroviruses (e.g., XMRV) Early studies suggested an association between the retrovirus XMRV and ME/CFS, but this link has been discredited by subsequent research and retraction of the original findings2.
Model
It is well known that virus will alter the microbiome. This alteration is to trick/hijack the microbiome to produce chemicals/metabolites that the virus needs (and to reduce those that hurt it) [SEE BOTTOM FOR CLARITY]. Once the virus is eliminated, then sometimes the microbiome gets “stuck” in this state. People have symptoms of the virus (symptoms caused by the metabolites!) but do not have the virus any more.
It is this persistent change of the microbiome: dysbiosis; that I believe is the path to relief and possible remission.
Virus and Microbiome Treatment
Using herbs know to be both anti-viral and anti-bacterial is my favored approach. You may get severe die-off from these (along with a herxheimer effect). Die off will usually start to ebb by day 10-14 after starting.
My personal favorites are:
Tulsi
Haritaki
Neem
Wormwood (Artemisia)
Olive Leaf
The list of Anti-viral herbs
Herb
Notable Antiviral Actions
Tulsi (Holy Basil)
Herpes, hepatitis, influenza, coronaviruses Inhibits viral replication and modulates immunity28.
Neem
Herpes simplex virus (HSV-1 and HSV-2)27, Influenza viruses:10, Dengue virus:58, Hepatitis C virus (HCV)6, Coxsackie virus, polio, and HIV57, SARS-CoV-2 (COVID-19)49.
Olive Leaf
Inhibit viruses such as herpes simplex virus (HSV), influenza virus, hepatitis B and C, human papillomavirus (HPV), HIV, and notably, SARS-CoV-2 (the virus causing COVID-19)125678.
Haritaki (Terminalia chebula)
Antiviral activity against a range of viruses, including SARS-CoV-2 (the virus responsible for COVID-19), herpes simplex virus type 2 (HSV-2), and influenza A virus. In particular, Haritaki demonstrated inhibition of the SARS-CoV-2 main protease in laboratory assays, suggesting it may halt viral replication15.
Curcumin (from turmeric):
Antiviral against influenza, HIV, hepatitis, and coronaviruses8.
Ginseng:
Traditional use for immune support and antiviral activity5
Sage
HIV-1, herpes simplex, Indiana vesiculovirus Rich in safficinolide and diterpenoids; active against HIV-1, herpes simplex virus, and Indiana vesiculovirus157.
Oregano
Rotavirus, norovirus, general antiviral Contains carvacrol and thymol; effective against rotavirus, norovirus, and other viruses1578.
Fennel
Herpes, respiratory viruses Contains trans-anethole; shown activity against herpes viruses and respiratory viruses27.
Peppermint (Mentha piperita):
Contains menthol and rosmarinic acid; antiviral against herpes simplex and influenza viruses2.
Lemon balm
Herpes simplex, respiratory viruses Contains flavonoids and essential oils; active against herpes simplex and respiratory viruses7.
Ginger
Influenza, RSV, calicivirus Contains gingerols and zingerone; effective against influenza, RSV, and feline calicivirus5.
Garlic
Influenza, HIV, HSV-1, rhinovirus Contains allicin; antiviral against influenza, HIV, HSV-1, viral pneumonia, and rhinovirus53.
Echinacea
Colds, respiratory infections Boosts immune function and reduces duration of colds and respiratory infections8.
Elderberry
Influenza, cold viruses Traditionally used for influenza and cold viruses1.
Astragalus
General antiviral, immune boost Immunomodulatory and antiviral properties1.
Aloe vera
Coronaviruses, herpes, influenza, HPV Contains compounds effective against coronaviruses, herpes, influenza, HPV, and more2.
Thyme
Herpes, influenza, general antiviral Contains thymol and carvacrol; antiviral and antimicrobial7.
Andrographis
Influenza, hepatitis C, dengue Contains andrographolide; active against influenza, hepatitis C, and dengue8.
Artemisia annua (Wormwood)
Hepatitis B & C, malaria Used for malaria; also shows antiviral activity against hepatitis B and C48.
My Personal Protocol
Do one at a time for 7-14 days, then move to the next one. Take notes on die-off or symptom changes with each. Constant rotation is strongly encouraged. Repeat but with only that cause a die-off or change.
You may or may not have a virus or re-activated virus. Most ME/CFS patients are not tested for all of the candidates virus listed above. Prescription antivirals with ME/CFS are very sensitive to which virus that a person has.
Appendix
Viruses lack their own metabolic machinery and rely entirely on host cell metabolites and metabolic pathways to reproduce. While viruses do not carry out metabolism independently, they hijack and reprogram the host cell’s metabolic processes to obtain the energy, nucleotides, lipids, and amino acids required for replication. Key findings include:
Metabolic Reprogramming by Viruses
Aerobic glycolysis (Warburg effect): Most viruses induce glycolysis to rapidly generate ATP and intermediates like pyruvate/lactate, even in oxygen-rich conditions12. This provides energy and substrates for viral genome replication (e.g., nucleotides from glucose metabolism)13.
Nucleotide production: Viruses like HSV-1 redirect the pentose phosphate pathway and TCA cycle to boost purine/pyrimidine synthesis for genome replication3.
Host Dependency Examples
Human cytomegalovirus (HCMV) increases glycolytic flux, TCA cycle intermediates, and fatty acid synthesis to support its 96-hour replication cycle13.
Herpes simplex virus (HSV) prioritizes nucleotide synthesis over glycolysis, reflecting its faster 24-hour replication timeline3.
SARS-CoV-2 hijacks folate metabolism and one-carbon pathways to facilitate RNA synthesis6. Inhibiting these pathways reduces viral replication.
Experimental Evidence
Glycolysis inhibitors like 2-deoxyglucose (2-DG) block late-stage herpesvirus assembly1.
Adenovirus activates Myc oncogene signaling to drive glycolysis and nucleotide synthesis1.
Vaccinia virus is an exception, showing minimal glycolysis dependence and instead utilizing alternative carbon sources like sorbitol1.
In summary, viruses co-opt host metabolites by reprogramming cellular metabolism to meet their replication demands. This metabolic hijacking is a nearly universal feature of viral reproduction, making host metabolic pathways potential therapeutic targets126.
My focus for the last few years has been on the ME/CFS Microbiome. I decided to test a variety of AI sites for their answering of the question below. Why do I ask this question? Simple, the rate of ME/CFS is very different between men and women, hence the differences of the microbiome may account for this.
What is the difference of reference ranges between 30 year old men and women microbiomes
Women may have more short-chain fatty acid (SCFA) producers (Roseburia, Faecalibacterium), influencing metabolism.
Men may have more bile-tolerant bacteria (Bilophila), linked to high-fat diets.
Perplexity.com
Alpha Diversity
Women generally exhibit higher microbial richness (SV richness) and Shannon diversity indices compared to men in young adulthood,
Taxonomic Composition
Females show higher abundances of Bacteroides, Prevotella, and Faecalibacterium, while males tend to have more Clostridium clusters and Enterobacteriaceae124.
Diversity: Some studies suggest that women in their younger adult years (including around age 30) tend to have a higher alpha diversity (a measure of the variety of species within an individual) in their gut microbiome compared to men of the same age.
Claude 3.7 Sonnet
Key microbiome differences between 30-year-old men and women:
Bacterial diversity: Women often show slightly higher overall microbial diversity
Firmicutes/Bacteroidetes ratio: Men typically have higher levels of Bacteroidetes, while women tend to have higher levels of Firmicutes
Sex-hormone influenced taxa: Women generally have higher abundance of Akkermansia, Bifidobacterium, and certain Lactobacillus species
Bile acid metabolism: Different bile acid profiles between sexes influence microbiome composition
Prevotella vs. Bacteroides: Women often show higher relative abundance of Prevotella compared to men
Grok.com
Women: Higher relative abundance of Firmicutes and Actinobacteria, lower Bacteroidetes. This may contribute to a higher Firmicutes/Bacteroidetes (F/B) ratio, associated with energy extraction from food. Premenopausal women show enriched species like Bifidobacterium, Ruminococcus, and Akkermansia, which are linked to beneficial metabolic effects.Men: Higher Bacteroidetes (e.g., Bacteroides, Prevotella), with men three times more likely to have a stool community type dominated by Prevotella over Bacteroides.
At age 30, women generally show higher gut and oral microbiome diversity, with enriched Firmicutes and Actinobacteria in the gut and Lactobacillus-dominated vaginal microbiomes. Men have higher skin microbiome diversity and gut Bacteroidetes abundance. These differences stem from hormonal and immune interactions, impacting disease susceptibility.
“Understanding these differences is essential, as they can have profound implications for health, particularly in conditions like irritable bowel syndrome (IBS) and metabolic disorders. “
“Research has shown that the microbiome of male mice exhibits higher levels of Firmicutes and lower levels of Bacteroidetes compared to females, contributing to differences in health outcomes and susceptibility to diseases such as CRC”
None of the other bacteria listed below were reference. Lots of discussion on hormones. The response was disappointing.
ChatGPT.com
Similar to DeepSeek above (not a surprise!).
Relative Abundances of Bacterial Genera (typical trends):
Bacterial Genus
More Abundant In
Notes
Bacteroides
Men
Linked with protein and fat-rich diets
Prevotella
Women
Often higher in fiber-rich diets
Akkermansia
Women
Linked to estrogen levels; supports mucosal health
Faecalibacterium
Both
Anti-inflammatory, usually similar in healthy individuals
And this summary
Feature
Men
Women
Microbial diversity
Lower
Higher
Dominant genus
Bacteroides
Prevotella, Lactobacillus
Hormonal effect
Lower
Higher
Butyrate production
Lower
Higher
Bottom Line
Differences were cited for the following bacteria. I suspect everyone has been reported in one or another study. All of the AIs appear to have incomplete answers. Incompleteness is expected, given their methodology of assembling data. The knowledge level is likely typical of most medical professional: reflecting what they have recently read (and not the entire body of available literature)
It was interesting to note that some of the differences were ascribed to male or female eating habits.
My great disappointment is that no microbiome testing company that I am aware of, uses reference ranges that are gender and age based. That makes identifying truly abnormal shifts questionable.
To give a practical example, suppose that you are getting reference range for height instead. You measure people on the street (it happens to be in front of shipyard). We know women tend to be up to 14cm shorter than men, so a bias to males in your sample is ignored. If the shipyard is in India, you get 154 cm. In Holland, 184 cm. So conclusions about a person having “stunted growth” or “excessive growth” based on their height without any reference to appropriate context becomes very suspect. A female that is 140 cm in India could be deemed to have stunted growth — yet is the average height for a woman in India.
I’d love some additional help, please. I’ve done two BiomeSight.com tests. I followed the suggestions after the first test and my microbiome has changed and some of my symptoms are improving. However, I couldn’t tolerate any of the bifidobacterium strains I tried, all of them caused very painful long-lasting migraines. Despite taking them for a combined 6wks (3 different strains for 2wks each), my bifidobacterium levels look unchanged. The suggestions do say that ‘No Probiotics without some adverse risks could not be identified.’ so maybe it’s better I just avoid them altogether for now?
I was diagnosed with ME/CFS 16yrs ago, after EBV 22yrs ago.
I caught Covid-19 in 2023.
I was diagnosed with chronic migraines in 2024 – they have increased in severity and occurrence over the last 5yrs, since the Covid-19 vaccines, though I can’t be sure it’s related.
My primary symptoms are: fatigue, pem, migraines, brain fog, ibs, acne, and hair loss.
I give my permission to use the above information anonymously for a blog post.
Analysis
I smiled when I saw ” ‘No Probiotics without some adverse risks could not be identified” and “I couldn’t tolerate any of the bifidobacterium strains I tried“. It seems that the expert system are making good (probable) suggestions. Suggestions are based on odds and not guaranteed.
Pass 1 – Based on Reported Symptoms
When there are many symptoms, my usual path is to get symptoms entered and then get suggestions focused on the bacteria likely associated to those symptoms. This is a targeted approach.
This person had entered any symptoms for their latest sample, and did for the sample from 7 months prior. 4-9 months between samples is what I advocate (balancing costs and time to change the microbiome).
I usually check all of the types of suggestions (I have no ideological position against using any of the types)
Then on the resulting page we see 12 bacteria that are the most likely causes. 2 low and 10 high. Suggestions are computed using five(5) different algorithms and then we use Monte Carlo Model to improve the odds of making good choices. Why different algorithms — simple, microbiome tests are fuzzy in their identification and many different criteria for selecting bacteria are advocated in the literature.
We go to the Consensus Suggestions and sort by Take Count — to get what all agrees about.
Looking at positive 5’s only:
Vitamins
Vitamin B2
Vitamin B1
Zinc
Amino Acid
Melatonin
Carnitine
Glutamine
Taurien
Antibiotic (Only 5’s)
loperamide hydrochloride Loperamide is most commonly used to treat acute and chronic diarrhea, including traveler’s diarrhea and diarrhea associated with inflammatory bowel disease (IBD).
florfenicol. Florfenicol is effective against a wide range of bacterial pathogens in animals, including both Gram-positive and Gram-negative bacteria. It is commonly used to treat respiratory infections, gastrointestinal infections, urinary tract infections, and other bacterial infections in livestock and companion animals
AtorvastatinAtorvastatin belongs to a class of medications known as statins, which work by inhibiting HMG-CoA reductase, an enzyme involved in cholesterol synthesis. By reducing cholesterol production in the liver, atorvastatin helps lower total cholesterol, LDL cholesterol (often referred to as “bad” cholesterol), and triglyceride levels.
It is interesting that Lactobacillus dominate with just one Bifidobacterium. I would carefully try these, one at a time, starting with a low dosage and increases, then change every 1-2 week to the next (keeping notes!!!), My preferred source of probiotics are listed here.
Pass 2 – Based on PubMed
I view this method as less accurate but the suggestions are ideal for discussion with a MD if antibiotics or other prescription items are suggested. It is available as the last item.
Rather than detailing items, I attached the report below
I’ll give this new round of suggestions a go, and then I’ll do another test.
I don’t have a willing GP (or vet, lol) to prescribe antibiotics but it’s very interesting that statins suggested – high cholesterol runs in my family and a lot of them are on statins.
The cholesterol issues are often DNA related… and DNA also impacts the microbiome. DNA is hard to change, the microbiome is easier.
From Perplexity: High cholesterol levels can indeed be influenced by genetic factors, with both common and rare gene variants playing significant roles in LDL cholesterol regulation. Here’s a breakdown of the genetic mechanisms involved:
Key Genes Affecting Cholesterol
LDLR (LDL Receptor) Mutations in this gene (chromosome 19) disrupt LDL cholesterol clearance, causing familial hypercholesterolemia (FH). This autosomal dominant condition leads to lifelong elevated LDL levels (200–300% higher in heterozygotes) due to defective receptor production or function126.
APOB (Apolipoprotein B) Mutations in APOB impair LDL binding to receptors, reducing clearance. For example, the APOB variant causing “familial ligand-defective apoB-100” increases LDL by 200–300%17.
PCSK9 Gain-of-function mutations in this gene degrade LDL receptors excessively, raising LDL levels. Conversely, loss-of-function variants (e.g., in 2% of African Americans) lower LDL by 30% and protect against heart disease168.
E4 carriers have ~5% higher LDL due to rapid lipoprotein clearance and LDLR downregulation.
E2 carriers have ~5% lower LDL but risk familial dysbetalipoproteinemia13.
Inherited Disorders
Familial Hypercholesterolemia (FH): Caused by mutations in LDLR, APOB, or PCSK9. Affects ~1/250 people, leading to LDL >190 mg/dL and premature atherosclerosis if untreated146.
Familial Hypobetalipoproteinemia: APOB mutations reduce LDL production, resulting in very low cholesterol levels13.
Autosomal Recessive Hypercholesterolemia: Rare ARH mutations cause LDL receptor dysfunction, leading to severe cholesterol elevation1.
Polygenic Influences
Most hypercholesterolemia cases involve interactions between multiple common variants (e.g., APOE, NPC1L1) and lifestyle factors. These variants individually exert small effects but collectively contribute to cholesterol variability137.
While genetics set baseline risks, diet and exercise remain critical for management, especially in individuals with predisposing variants368. Genetic testing is recommended for suspected FH to guide early intervention
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
First, apologies to people over the microbiome prescription site being up, then down, then up, then down. The hosting company that I am using (and 900,000 other customers!) having been dealing with issues with their cloud provider. As I write this on Saturday, March 8th 2025, evening — it is back up.
Today, I reworked some old page concepts, improving the mathematics and the presentation. The purpose is to give you some ideas of where your ME/CFS or Long COVID may progress. By progress, I mean symptoms that may get added to your already massive list.
This will show a page with no symptoms/characteristics entered.
Enter the most critical symptom that you have. For this example, I will do long COVID. Just enter it in the Search box until you see what you are interested in
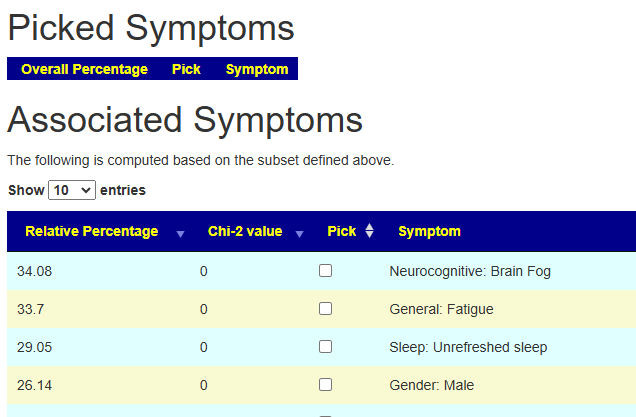
Check the Check box and the page will refresh. You will see that 11.7% of the samples report Long Covid. Below it are the OTHER symptoms that these people report — with the percentage that reports each symptom
We will pick POTS next. The page will update. Note that Post exertional Malaise that was 26% chance above jumps to 67%. Having POTS with Long COVID increases the odds.
Adding in General Headaches, increases Brain Fog to 84% chance. If you do not have Brain Fog at the moment, there is a very good chance that you will get it.
Bottom Line
The purpose of this tool is give concrete odd of what your next symptoms may be. Here’s a walk through.