This is the title of a new publication in Microbes & Immunity, available here.
Microbiome fluctuations or metabolic endotoxemia are proposed as possible disorder biomarkers. Based on the fact that gut microbiota dysbiosis reverts to a state of eubiosis in long-term patients with this condition, it may be hypothesized that disease progression begins with the loss of beneficial gut microorganisms, particularly short-chain fatty acid producers, leading to more widespread gastrointestinal phenotypes that are subsequently reflected in plasma metabolite levels. These alterations, specific of each individual, thereby result in metabolic and phenotypic shifts and in ME/CFS.
This has been my primary hypothesis for many years and lead to my writing Microbiome Prescription to normalize the dysbiosis. The bacteria shifts will be reported differently from different labs because of a lack of standardization of microbiome tests (See The taxonomy nightmare before Christmas… ).
Below I have pulled the lab specific dysbiosis shifts for ME/CFS at thhe genus level.
Biomesight Tests
The number are the percentile ranking for the bacteria listed. Each match increases the odds of ME/CFS by 1.5.
Methylonatrum >= 99
Planifilum >= 98.9
Thiohalorhabdus >= 98.9
Granulicatella >= 98.7
Amedibacillus >= 98.6
Enterococcus >= 98
Methylobacillus >= 98
Emticicia >= 97.7
Candidatus Tammella >= 97.7
Dokdonella >= 97.6
Runella >= 97.4
Collinsella <= 18
Pseudobutyrivibrio <= 16.4
Calothrix <= 13.8
Lachnospira <= 11.4
Veillonella <= 10.8
Shuttleworthia <= 8.5
Parabacteroides <= 8.4
Bifidobacterium <= 8.4
Faecalibacterium <= 7.5
Actinobacillus <= 7.5
Pedobacter <= 7.2
Coprococcus <= 4.6
Moorella <= 3.5
Natronincola <= 2.9
Mediterraneibacter <= 2.5
Oscillospira <= 1.8
Anaerovibrio <= 1.7
Sphingobacterium <= 1.6
Thryve
Collinsella <= 44.2
Bifidobacterium <= 41.1
Gemmiger <= 23
Dorea <= 19
Butyrivibrio <= 8
Fusicatenibacter <= 5.7
Lachnoclostridium <= 5.2
Gordonibacter <= 5.1
Eubacterium <= 4.8
Prevotella <= 4
Brassicibacter <= 3.9
Sporobacter <= 3.5
Johnsonella <= 3.5
Phascolarctobacterium <= 3.4
Dialister <= 3.4
Agathobacter <= 3.3
Lactonifactor <= 3.2
Murimonas <= 3.2
Moryella <= 3.1
Niabella <= 3.1
Ruminococcus <= 3
Hungatella <= 3
Anaerotruncus <= 2.8
Odoribacter <= 2.7
Lactobacillus <= 2.4
Eggerthella <= 2.3
Cellulosilyticum <= 2.1
Haemophilus <= 2
Holdemania <= 2
Terrisporobacter <= 2
Anaerobutyricum <= 1.9
Howardella <= 1.8
Hydrogenoanaerobacterium <= 1.8
Lachnobacterium <= 1.8
Hespellia <= 1.7
Agathobaculum <= 1.6
Pseudoflavonifractor <= 1.6
Desulfotomaculum <= 1.6
Intestinibacter <= 1.6
Barnesiella <= 1.5
Eisenbergiella <= 1.5
Facklamia <= 1.5
Acetatifactor <= 1.5
Ruminiclostridium <= 1.5
Natranaerovirga <= 1.5
Enterocloster <= 1.4
Caloramator <= 1.4
Thomasclavelia <= 1.4
Desulfovibrio <= 1.4
Parabacteroides <= 1.4
Shuttleworthia <= 1.3
Peptoniphilus <= 1.3
Akkermansia <= 1.3
Alistipes <= 1.3
Marvinbryantia <= 1.3
Acetivibrio <= 1.2
Paraprevotella <= 1.2
Veillonella <= 1.2
Bacteroides <= 1.2
Butyricimonas <= 1.2
Romboutsia <= 1.2
Ethanoligenens <= 1.2
Phocaeicola <= 1.2
Anaerocolumna <= 1.2
Blautia <= 1.1
Coprococcus <= 1
Lachnospira <= 1
uBiome
Veillonella <= 22.4
Hespellia <= 19
Bifidobacterium <= 15.1
Anaerosporobacter <= 7.2
Streptococcus <= 6.8
Eggerthella <= 6.4
Phascolarctobacterium <= 4.1
Eisenbergiella <= 3.9
Marvinbryantia <= 3.4
Holdemania <= 3.1
Dorea <= 3
Anaerostipes <= 3
Oscillibacter <= 2.7
Dialister <= 2.3
Kluyvera <= 2.1
Peptoclostridium <= 1.7
Erysipelatoclostridium <= 1.4
Intestinimonas <= 1.3
Sarcina <= 1.3
Roseburia <= 1.3
Phocaeicola <= 1.2
Terrisporobacter <= 1.2
Bacteroides <= 1.1
Bottom Line
Bifidobacterium is common across all of these, and lactobacillus shows up barely in only one result. Since there can be some hostility between Bifidobacterium and Lactobacillus, I would suggest cutting out lactobacillus probiotics.
I repeated this for Bifidobacterium species and one species shone.
Bifidobacterium longum <= 9.9
My personal preference for a source is Maple Life Science which sells direct from factory resulting in very fresh and alive probiotics.
Some examples of analysis people with Long COVID and ME/CFS are there. I am working on building an algorithm to build suggestions based on odds ratio which should improve the suggestions more.
Some supplements that I have been taking since the last test:
Tetracycline
Clove
Holy basil (Neem)
Augmentin + Bromelain
Grapefruit seed extract
Monolaurin
Apple peel powder
Thyme
My symptoms:
Still get the red nose (some form of rosacea).
Still feel fatigued (both physically and mentally). But it is better than before.
Feeling stressed. But it is better than before.
Brain fog.
Bloated.
Lots of gas – I fart and burps a lot.
Issues with allergies (itching eyes, stuffed nose and itchy skin)
Video
Analysis
We will start with the high-level comparison. Note that some numbers will change with time. There are no major changes. Since the latest sample reports 20% more bacteria, many counts are expected to be 20% higher – for example: Thorne Ranges: old: 230 + 20% = 276, with the seen count being 253 (so an apparent improvement although the number went up)
Criteria
9/2/2024
1/22/2024
9/12/2023
2/22/2023
8/11/2022
3/25/2022
12/3/2021
8/31/2021
Lab Read Quality
9.1
7.9
3.5
9.7
5.5
6.2
3.6
7.8
Outside Range from GanzImmun Diagostics
16
16
16
15
15
17
17
20
Outside Range from Lab Teletest
23
20
20
24
24
22
22
25
Outside Range from Medivere
14
16
16
15
15
15
15
19
Outside Range from Metagenomics
6
7
7
9
9
7
7
8
Outside Range from Microba Co-Biome
3
2
2
7
7
1
1
1
Outside Range from MyBioma
6
5
5
7
7
7
7
8
Outside Range from Nirvana/CosmosId
21
20
20
23
23
18
18
21
Outside Range from Thorne (20/80%ile)
253
230
198
223
223
217
217
246
Outside Range from XenoGene
32
32
24
32
32
36
36
39
Outside Lab Range (+/- 1.96SD)
12
5
15
10
11
9
9
14
Outside Box-Plot-Whiskers
48
52
56
42
36
42
59
42
Outside Kaltoft-Moldrup
113
123
70
139
56
78
59
140
Bacteria Reported By Lab
600
508
399
666
478
613
456
572
Bacteria Over 85%ile
48
52
Bacteria Under 15%ile
118
157
Pathogens
23
26
25
30
23
39
24
30
Condition Est. Over 85%ile
2
5
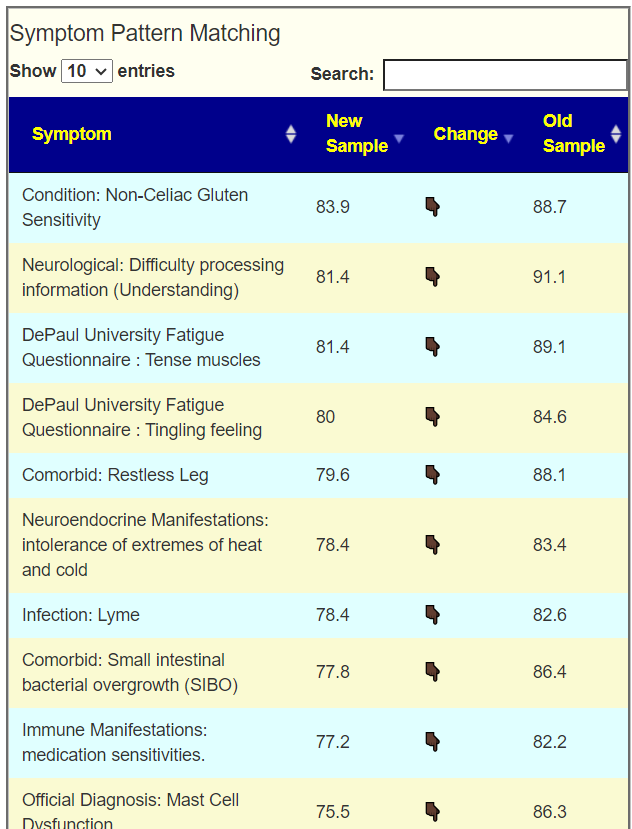
There is a new comparison table added that compares sets of symptoms bacteria for symptoms reported in either sample. This is a thought experiment on a different way of evaluating the microbiome, i.e. are symptom bacteria reducing. Remembering that we have 20% more bacteria reported, the improvement may be slightly under-reported.
Going Forward
My current preference is to use symptom associations suggestions with KEGG suggested suggestions. This assumes that the person has added their symptoms.
Using Entered symptoms
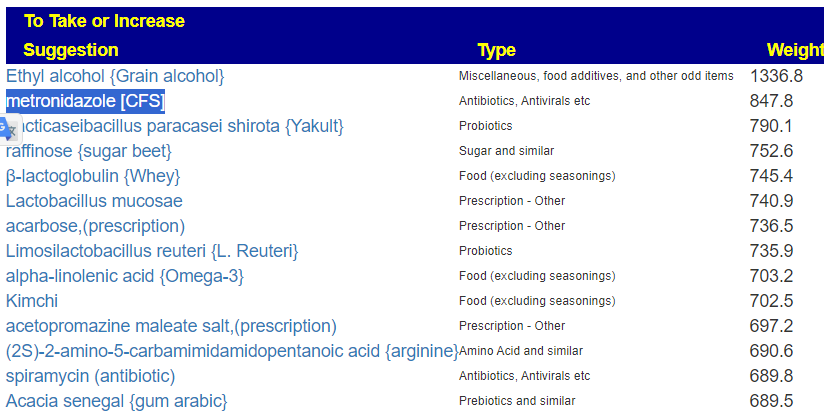
Since this person has access to antibiotics, I opted to include all classes of modifiers. We have 38 bacteria selected — a reasonable number
The suggests were a nice mixture for ME/CFS. Typically, I see the top being just antibiotics, in this case we have several probiotics there.
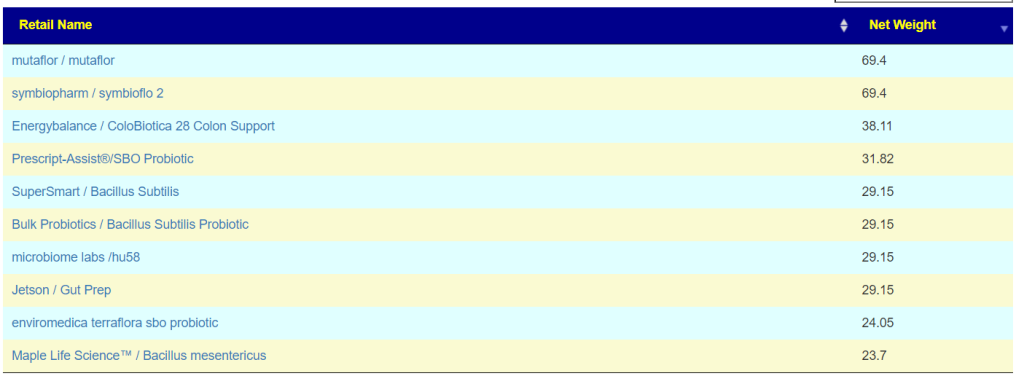
And suggested retail probiotics are:
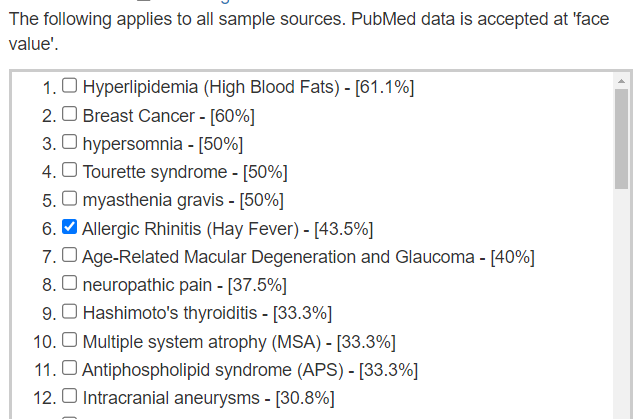
Using Diagnosis and PubMed
Using a diagnosis provides less precise filtering compounded by different labs (with different identification of bacteria). If the person is using a lab that lacks a large number of annotated samples from that lab, then it is the best path.
The suggested path is to go down the list and pick the ones that has the highest value(s) that agrees with one or more of the diagnoses that you have.
In this case we have only 4 bacteria in the selection, so the suggestions will be likely more generic than specific.
There are no antibiotics in this list
The probiotic list is below. It has some similarities to the above list.
Using KEGG Derived Probiotics
This is an experimental approach that attempts to do a metagnòmia approach from the available data. We estimate which compounds are too high or too low. Then we match them to probiotics which produce or consumes them. Postbiotics can be used for items that are too low. There is no filtering of any type; we look at the entire microbiome.
The results are different — as to be expected. Why expected? The prior ways depended on studies being done what each probiotics bacterium does. Often there are no studies. This way uses the DNA/RNA sequences of everything and thus we do not need studies.
I usually focus on too low, with the assumption that a surplus will just be ignored or has less impact (i.e. starvation versus obesity) We can see where there is agreement between the lists.
This can be made more complex by using consensus / Monte Carlo Model
Reader Plan
Microbiome Prescription produces suggestions, the weights/priorities are the odds of causing a change and not the amount of change (there is simply no objective data to compute the amount). This reader did their own evaluation of what they felt comfortable with (excellent idea).
I have also bought 2 more tests so I will do them with max 3 months apart as you said in the video.
I came up with this protocol by using the “Beginner-Symptoms: Select bacteria connected with symptoms”:
Week 1-2: Gum arabic
Week 3-4: Monolarin (lauric acid)
Week 5-6: Psyllium
Week 7-8: Rosemary
Week 9-10: Parsley
Week 11-12: SymbioFlor-2
I found that I get best results from herbs, prebiotics and antibiotics. The only probiotic I’ve got good results from is Symbioflor 2 (an E.Coli probiotic) [Editor: E.Coli probiotics also worked best for me]
A lot of probiotics that I’ve tested I’ve got bad results from.
Postscript and Reminder
As a statistician with relevant degrees and professional memberships, I present data and statistical models for evaluation by medical professionals. I am not a licensed medical practitioner and must adhere to strict laws regarding the appearance of practicing medicine. My work focuses on academic models and scientific language, particularly statistics. I cannot provide direct medical advice or tell individuals what to take or avoid.My analyses aim to inform about items that statistically show better odds of improving the microbiome. All suggestions should be reviewed by a qualified medical professional before implementation. The information provided describes my logic and thinking and is not intended as personal medical advice. Always consult with your knowledgeable healthcare provider.
Implementation Strategies
Rotate bacteria inhibitors (antibiotics, herbs, probiotics) every 1-2 weeks
Some herbs/spices are compatible with probiotics (e.g., Wormwood with Bifidobacteria)
Verify dosages against reliable sources or research studies, not commercial product labels. This Dosages page may help.
My preferred provider for herbs etc is Maple Life Science™ – they are all organic, fresh, without fillers, and very reasonably priced.
Professional Medical Review Recommended
Individual health conditions may make some suggestions inappropriate. Mind Mood Microbes outlines some of what her consultation service considers: A comprehensive medical assessment should consider:
Terrain-related data
Signs of low stomach acid, pancreatic function, bile production, etc.
Detailed health history
Specific symptom characteristics (e.g., type and location of bloating)
From a reader. His prior microbiome analysis is here.
A short update…
About two months ago I had a sinus infection and got a week long course of Amoxicillin for it. Almost all my symptoms went away during the antibiotic treatment.
Each day I was just waiting to get to take my daily dose, the improvement was so substantial.
After finishing the course, it took about 48 hours until I was pretty much back to where I started.
After the treatment stopped, the symptoms came back. Nothing changed in the end.
But while on the treatment I felt great. I slept fantastic. All my pain went away. All my tired and wired symptoms went away. But the improvement did not persist.
Two weeks ago I went to see a doc that I know fairly well, and told him what happened. After hearing my story, he gave me a month long treatment of Doxycycline. I do not know his rationale for not giving me Amoxicillin.
Many years ago I also had a lung infection and was treated with Ciprofloxacin. It also removed the symptoms during treatment.
The Doxycycline does nothing for my symptoms. It only creates an upset stomach, when Amoxicillin gave me no side effects except curing my CFS and MCS.
Why does Amoxicillin help, but Doxycycline not? But not Doxycycline..the one antibiotic I managed to get a lot of..but it does not help.
Are there any conclusions to be drawn from this information?
We have this person’s microbiome uploaded, so first step is to just run “Just Give Me Suggestions”
I then using the available data for these three to see what the other two does not — i.e. the smoking gun
Taxa Name
Taxa Rank
Enterobacteriaceae
family
Moraxellaceae
family
Enterococcaceae
family
Aeromonadaceae
family
Pseudomonadaceae
family
Verrucomicrobiaceae
family
Morganellaceae
family
Atlantibacter
genus
Metakosakonia
genus
Pseudescherichia
genus
Limnobaculum
genus
Lelliottia
genus
Pluralibacter
genus
Kosakonia
genus
Shimwellia
genus
Roseimicrobium
genus
Rosenbergiella
genus
Brevifollis
genus
Pseudocitrobacter
genus
Franconibacter
genus
Siccibacter
genus
Gibbsiella
genus
Candidatus Moranella
genus
Candidatus Schneideria
genus
Candidatus Profftia
genus
Candidatus Riesia
genus
Candidatus Ishikawaella
genus
Cronobacter
genus
Phytobacter
genus
Mangrovibacter
genus
Biostraticola
genus
Luteolibacter
genus
Persicirhabdus
genus
Candidatus Regiella
genus
Haloferula
genus
Buttiauxella
genus
Leclercia
genus
Cedecea
genus
Trabulsiella
genus
Yokenella
genus
Raoultella
genus
Fucophilus
genus
Acinetobacter
genus
Pseudomonas
genus
Prosthecobacter
genus
Candidatus Phlomobacter
genus
Citrobacter
genus
Enterobacter
genus
Klebsiella
genus
Kluyvera
genus
Morganella
genus
Proteus
genus
Salmonella
genus
Shigella
genus
Aeromonas
genus
Plesiomonas
genus
Enterococcus
genus
Verrucomicrobium
genus
Scandinavium
genus
Jejubacter
genus
Sulfuriroseicoccus
genus
Entomohabitans
genus
Next, we look at his last sample for these and found:
Taxa Name
Tax Rank
Percentile
Enterobacter
genus
73.64152
Enterococcus
genus
69.35996
Lelliottia
genus
68.33713
Enterococcaceae
family
62.73872
Enterobacteriaceae
family
60.38241
Enterobacterales
order
59.50287
Klebsiella
genus
54.63183
Klebsiella/Raoultella group
no rank
54.63183
Pseudomonadaceae
family
41.17647
Pseudomonas
genus
41.0804
Verrucomicrobiaceae
family
21.69038
Verrucomicrobiales
order
19.43128
Aeromonadaceae
family
17.55486
Moraxellaceae
family
14.05018
Next step is to look at the combinations of these top 3 bacteria to see how they rank (percentile) in combination
Enterobacter,Enterococcus – 72%ile
Enterococcus, Lelliottia – 75%ile
Enterobacter, Lelliottia – 74%ile
Enterobacter, Enterococcus, Lelliottia – 79%ile
The presence of Lelliottia makes things marginally more significant.
Looking at the Taxa Tree
One possibility is that the cause of not a genus that is reported with 16s tests. Looking at the tree we can determine the “unknowns” The Family is 910 from which we remove (150,70,230,40,10) ending with 410 unclassified i.e. almost half of the bacteria in Enterobacterales are not identified. Any smoking gun may be hidden in the deficiencies of 16s testing.
Where we are
We do not know precisely the bacteria involved with ME/CFS and MCS. For this person, the antibiotic history does allow us to identify possible candidates. The next question is obvious, which antibiotics should we suggest to the MD? We have the consensus list and we want to reduce it to those that impact these three bacteria as the most likely to help.
For all three bacteria, we have the following list (Note that the [CFS] indicates that it is often used by ME/CFS Specialists)
Weight
Antibiotic
769.5
tobramycin (antibiotic)s
608.2
amikacin (antibiotic)s
590.4
amoxicillin (antibiotic)s[CFS]
563.5
gentamicin (antibiotic)s
441.6
imipenem (antibiotic)s
388.6
streptomycin (antibiotic)s
380.1
erythromycin (antibiotic)s[CFS]
326.5
azithromycin,(antibiotic)s[CFS]
301.6
intesti-bacteriophage
261.3
vancomycin (antibiotic)[CFS]
191.2
ciprofloxacin (antibiotic)s[CFS]
178.7
clarithromycin (antibiotic)s[CFS]
86.5
rifaximin (antibiotic)s
81.2
carbapenem (antibiotic)s
The challenge is now persuading the MD to prescribe these based on the microbiome sample and this analysis. Next we look at alternatives.
Non Prescription Approaches
As above, we restrict to those items that reduces all three of the above bacteria
ALL probiotics were negative
Nothing for Amino Acid and similar
Nothing for Prebiotics and similar
Nothing for Food or Diet Style
Nothing for Vitamins and Minerals (Vitamin B2 was just a 2)
Hesperidin (polyphenol) – was over 800 and the only Flavonoids, polyphenols with a positive value
N-Acetyl Cysteine (NAC) – was over 700 and the sole common supplement
chitosan,(sugar) – was 200’s and the sole sugar
Herbs and Spices
I have also been trying multiple different herbs. The one which so far has given the best effect is an alcoholic tincture of Artemisia Annua.
From reader
Wormwood(artemisia) is a 21 (minor positive impact predicted). It reduces some genus of Enterobacteriaceae but nothing reported for Enterococcus, Lelliottia or Enterobacter.
Priority
Modifier
329.4
foeniculum vulgare,fennel
294.4
laser trilobum l.,kefe cumin
289.6
hypericin, St. John’s Wort
213.1
neem
164.6
tulsi
118.7
garlic (allium sativum)
105.9
Curcumin
23.6
triphala
-20.5
cinnamon (oil. spice)
-49.6
oregano (origanum vulgare, oil) |
-87.4
persimmon tannin
-143.2
Dangshen
-313.3
berberine
Suggestions to discuss with MD
If antibiotics are not viable then the following seems to be the best choices
Hesperidin (polyphenol)
N-Acetyl Cysteine (NAC)
Foeniculum Vulgare, Fennel
laser trilobum l.,kefe cumin
Hypericin, St. John’s Wort
Neem
Hesperidin..very interesting herb. It says to assist with blood flow and blood vessel health, exactly the type of issues I am dealing with. I will try it.
Feedback from person on draft
Bottom Line
This was a very interesting post because we seem to be able to identify the family of bacteria involved with this person’s symptoms Enterobacteriaceae. This agrees with the literature.
“The prevalence and median values for serum IgA against the LPS of enterobacteria were significantly greater in patients with CFS than in normal volunteers and patients with partial CFS.” [2010]
“Often, a lower Bacteroides/Firmicutes ratio can be accompanied by an increase in Enterobacteriaceae, therefore suggesting a complete reshuffling of the gut microbiota composition” [2021]
“Increased Serum IgA and IgM against LPS of Enterobacteria in Chronic Fatigue Syndrome (CFS): Indication for the Involvement of Gram-Negative Enterobacteria in the Etiology of CFS and for the Presence of an Increased Gut-Intestinal Permeability” [2007]
I do have a concern that almost 50% of the genus in Enterobacteriaceae were not identified in the sample. We are in a bit of fog — which we will address by assuming it will also be sensitive to it sibling genus.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
If you search ME/CFS + the name of a developed country, and then others, you will find that nations with high HDI are dealing with a bizarre, chameleonic, epidemic and endemic disease, a debilitating, systemic, very serious condition in many cases, and associated to suicides – a disease that has an incredible and revealing history, and that is expanding in cities almost all over the world, especially in the West.
Although it is said that it is still not enough, there are initiatives in these countries by numerous foundations, NGOs, universities, health systems, social movements, professionals, clinics and laboratories, patient associations, and company programs, aimed at raising awareness, funding, and combating the disease. Recently ME/CFS was discussed in the German parliament, and yesterday I read that it will be part of the UK medical curriculum. Fantastic. I have been studying the disease for 18 years.
The Netherlands, Belgium, and the Scandinavian countries are also especially victimized by ME/CFS and similarly develop medical education, awareness, treatment, and prevention programs. In the highly evolved and cold Iceland, where epidemic outbreaks occurred, the disease was so prevalent that it acquired local names: neuromyasthenia, Akureyri’s disease, and later Iceland disease. In the United States, in 2008, ME/CFS was considered by the CDC as the most concerning public health problem in the country. In Canada, the prevalence is as high or greater than in the USA.
These are characteristics common to countries with a lot of ME/CFS, a high HDI, an abundance of industrialized (sterilized) food; and perhaps, very cold winters. In Oceania and Japan, the prevalence appears to be somewhat lower.
A map of ME/CFS epidemics published by Donald Acheson in 1959 already showed target countries; these have changed little, but the number of patients has exploded.
Acheson, E.D. (1959), The Clinical Syndrome Variously Called Benign Myalgic Encephalomyelitis, Iceland Disease and Epidemic Neuromyasthenia, American Journal of Medicine, 26 (4): 569–595
However, in developing nations the ME/CFS story is different. Let us see.
Search now ME/CFS + the name of a tropical developing country: you find nothing or almost nothing. In these countries, the disease is practically unknown, because, in fact, the number of people affected is relatively much smaller. But not just for that.
These numbers are repeated throughout Latin America, and most of Asia: ME/CFS in these regions is almost non-existent. In African nations, the prevalence is very low, with two exceptions: South Africa (where there is a high HDI and cold winters), and Nigeria, whose high prevalence of ME/CFS is attributed to endemic malaria; but which in my opinion is due more to the excessive or preventive use of antibiotics, due to the large number of infections of the water cycle.
Let’s consider Brazil, a continental country, with 215 million inhabitants, large metropolises, 546 thousand doctors, powerful advanced medicine, hospitals among the best on the planet, a gigantic public and universal health system, legal telemedicine, and 357 medical schools – the largest number of medical schools in the world. However, searching today (June 24, 2023) on Google using Chrome: ME/CFS + Brasil; I found only one paper from 2010 that mentions CFS, nothing else. No publication in the last thirteen years even mentions the acronym ME/CFS.
Using Microsoft’s Bing, I found only a brief discussion on a Forum (February 2021) outside of Brazil Brazil: ME/CFS in Brazil | Phoenix Rising ME/CFS Forums, which reported on the lack of awareness of the disease in the country; and revealed the launch of the country’s first website about the condition.
I participate in some groups of doctors; among 800 professionals, only six knew about the disease; two of them have the condition.
And why does this happen?
I understand there are four reasons:
1) The country’s medical culture ignores the existence of ME/CFS, setting up a classic example by Claude Bernard: the doctor does not know what he is looking for, and does not value what he finds;
2) many patients with ME/CFS are labeled as having fibromyalgia, and many others remain undiagnosed;
3) because there is much less disease; restricted to classes A|B, almost three women for every man; and …
4) due to prejudice from health professionals; resulting from lack of knowledge and the unresolved problem that each patient brings or represents; and that closes the vicious circle. Just to cite one example, months ago, a renowned cardiologist colleague confessed to me among friends and other colleagues: “I hate it when the patient says he has fibromyalgia! ”… And he added: “If I could avoid it, I wouldn’t even evaluate the patient.”
So it is. For fifteen years, in order to better identify and investigate 70 patients with ME/CFS, I had to see 201 patients whose main diagnosis was fibromyalgia; another 39 were diagnosed with Lyme, viral fatigue, chronic EBV, psychosis, etc. Only 20 had the initial diagnosis of ME/CFS, formulated by me.
ME/CFS is a disease of rich countries, yes; but not only of those. And don’t make the mistake of thinking that the number of ME/CFS victims in Brazil and other developing countries is negligible; in the most privileged parts of these countries thousands live under a high HDI; and similarly develop the condition and fill the most luxurious offices and the relatively new pain clinics.
Importantly, in early 2020, long before the coexistence of ME/CFS and Covid complications now known as Covid Longa was described, I foresaw what are now facts: that the incidence of ME/CFS would explode in the post-Covid world, and that sequelae or late effects of the coronavirus would add to, or confound with ME/CFS – that the pandemics would entangle.
The results of the research, the experience with the patients, and data from the literature make it necessary to recognize that the fundamental etiogenic factor for ME/CFS is the hostile environmental disturbance that leads to the breakdown of the greater symbiosis; understanding the greater symbiosis as the complex and vital relationship that we need to maintain with the microbial world, and which, when broken, imposes burdens on homeostasis and leads to the state of disease.
There are many examples of our dependence on flora. Doctors are aware of the bleeding problem that stems from antibiotics. These drugs reduce the population of bacteria in the intestine that produce vitamin K, which is needed for clotting proteins. Without these bacteria, without this vitamin, we can bleed.
By way of illustration, in an elegant post by Elena Panzeri, the infographic below reveals 35 metabolites of the microbiome that participate in the development, function, and integrity of the human brain.
by Elena Panzeri | LinkedIn
The list is another example of the vital principles that are provided by the microscopic creatures that surround us and that we carry along with us; whose scarcity, imbalance, or anomalous interaction in an inhospitable environment, leads to what we know as ME/CFS. It makes sense to assume that the same is true for all other organs and systems.
The paradox of a so-called incurable disease, which has a rate of 4% to 8% of spontaneous cures reinforces this conviction. These healings occur by re-establishing the great symbiosis – casual, deliberate, or professionally oriented.
Today I read an article in which the author advocates the need for caution in attempts to restore the microbiome in ME/CFS patients, with which I wholeheartedly agree; it is difficult. But I don’t agree with the viral illness that she advocates as the cause of illness.
The cause is the deprivation and destruction of beneficial microorganisms in the surroundings and in the lives of those affected. In other words, the cause is the victory of civilization in the stupid war imposed on the microorganisms on which we depend for life and health. Due to fear of infections, we resolved that we should destroy them all around us, malefic and benefic, in every way. The result is ME/CFS. Just do not see it who refuses to see.
I have already posted repeatedly here that, once installed, the ME/CFS is a heavy transatlantic that left its course carried away by a strong current; correcting its course is usually a slow, tiring, painful process.
What I call an antibiotic environment is an environment hostile to the microbiome of urban life, with a high standard of sanitation, excessive hygiene, chlorinated and fluoridated water, and reduced social contact. The antibiotic environment is in hospitals and in the lives of health professionals; it can start with surgical, aseptic birth, and expand into the lives of solitary people, small families, apartments without animals and plants; and in detergents and antiseptics in all their forms; in the excessive use of antibiotics and antifungals, deodorants, alcohol gel, mouthwashes; it is in fast food, and in sterile foods, mainly industrially processed ones, in the additives and agrochemicals added to those; in pasteurization, in UHT, in irradiated foods, in preserves, in canned goods.
There is an enormous amount of chemical and antibacterial substances in industrialized foods, and it is legitimate to believe that they damage our flora.
In human food, this friendly, green, ECO logo, with a natural, organic look, is the radura logo. It signals that your food has been irradiated.
Radura Logo | Irradiated food
Irradiation is the pasteurization of the 21st century.
Radiation does not remain in the product and theoretically irradiated food is not harmful; but the good it does is limited; it roasts the DNA of any form of life, it kills all fungi and bacteria; extends the validity and duration of products. Dairy products lose life (fermenters die), are plasticized, and get chemical flavorings for flavor; and the banana in the plastic wrapper lasts over a month on the shelf.
It is relevant information that ME/CFS does not exist in simple people, nor in the rural environment in Brazil.
The opposite of ME/CFS is life in the countryside, it’s in full houses, with real food, made by hands, with fresh ingredients. It is in the water of the rivers, in the garden and in the garden, in bare feet, in unprotected sex, on the beach, in craft beer, in wine, in domestic animals, in fresh milk, and in food fermented at home.
I have examples and testimonies of people who have been healed by lifestyle changes. The adoption of a probiotic lifestyle, which includes the consumption of various natural probiotics, gradually improves the clinical picture.
There is a video of the end of the pandemic, in which the famous Brazilian actor Lima Duarte recounts his childhood in which he would wake up with his father at dawn, to take the calf to the cow and be able to milk it. He says that it is the cow’s love for her calf that makes her release her milk; and prophesies that other pandemics will come because we are living wrong – that the cow’s love is missing in the milk from mechanical milking. And what is more serious, I add: cow and calf microbiomes are also missing, my dear.
ME/CFS is the apple of the eye of anyone who sells diagnoses and treatments, finances or carries out research, creates products, information, and technology to treat the symptoms of a so-called never-ending disease, which causes so much suffering – and which is also a vast and fertile ground for all kinds of quackery.
To avoid conflict of interest, all medical research work was pro bono. All patients were returned to the colleagues who referred them.
There is a giant sphinx of evidence showing that restricted access to the planet’s microbiome is the fundamental etiogenic factor of ME/CFS, but most scientists refuse to face this veritable monument of information.
Let us see a few things.
There are 63 recognized epidemics of the disease, 31 of which occurred in hospitals, just affecting health professionals. The first, in 1934, hit all 198 nurses and doctors at the Los Angeles County Hospital, but curiously, none of the patients admitted to the institution. Until today, the predilection of the disease for health professionals is an undisputed fact; why is that? …
The fact is, health professionals spend most of their lives in aseptic environments, where access to the natural microbiome is blocked. Mechanical barriers (masks, gloves, caps, sterile clothing, disposable aprons, safety glasses, shoe covers), chemicals (frequent washing of hands with detergents, abusive and continuous use of degerming agents (alcohol, chlorhexidine, iodine, hypochlorite, etc.), and even cultural behaviors block the access to beneficial microorganisms. In 2010, I saw in London the recommendation to avoid kisses on the cheeks and handshakes on hospital premises.
Taking the first epidemic of ME/CFS as a paradigm, in 1934 Pasteur had already demonstrated the bacterial origin of the infections, but penicillin was still not available, and the hospital had many infections; hygiene norms were therefore neurotic. In addition, foods were also strictly sterile, and there was a boom in spam and canned foods, considered safer because they were sterile (the occurrence of botulism in the first canned foods led the industry to intensify food sterilization systems in cans).
DeMeirleir et.al. advocate that the ingestion of metals by people living with dysbiosis triggers or aggravates ME/CFS, and the welds of the first cans contaminated the food they contained with toxic metals.
The other epidemics victimized human groups in relatively isolated or restricted coexistence: convents, military bases, schools, a ship, industries, groups of athletes, having in common few interpersonal contacts, and cafeterias with carefully sterile food, aiming at the prevention of food infections. I believe that cold winters also favor the emergence of disease, by limiting the expansion of the natural microbiome.
Besides, considering the Epidemiology of ME/CFS, summarized in Chapter 15, it solidifies the understanding that the greater symbiosis breakdown leads to this confusing spectrum of diseases.
Adding to this set of evidence is the fact that isolated cases of these diseases began to affect middle-aged upper-middle-class women: more acculturated mothers and grandmothers, with access to better sanitation, and higher hygienic standards; determined to make food safer (meaning sterile) for their children and grandchildren.
I am not refuting here any of the hundreds, perhaps thousands, of research that demonstrates countless pathophysiological mechanisms involved in ME/CFS (although many are refutable); I just focus on the essential condition that leads to the development of the disease: the war imposed by civilization on the microbiome of the blue planet.
I am sure that in the near future a good epidemiologist with access to the internet, and with some software or calculator, will confirm my theory; which supports and has been strengthened by the research I have carried out over fifteen years.
In addition, I envision the moment when artificial intelligence resources and/or a broader meta-analysis will seal this knowledge.
This sphinx will not devour me. Neither will those willing to accept the intuitive knowledge that deciphers it.