
A reader asked me to review and comment on their uBiome results (site). Finally, I have a few hours from excessive support activity to do it.
The Results Summary
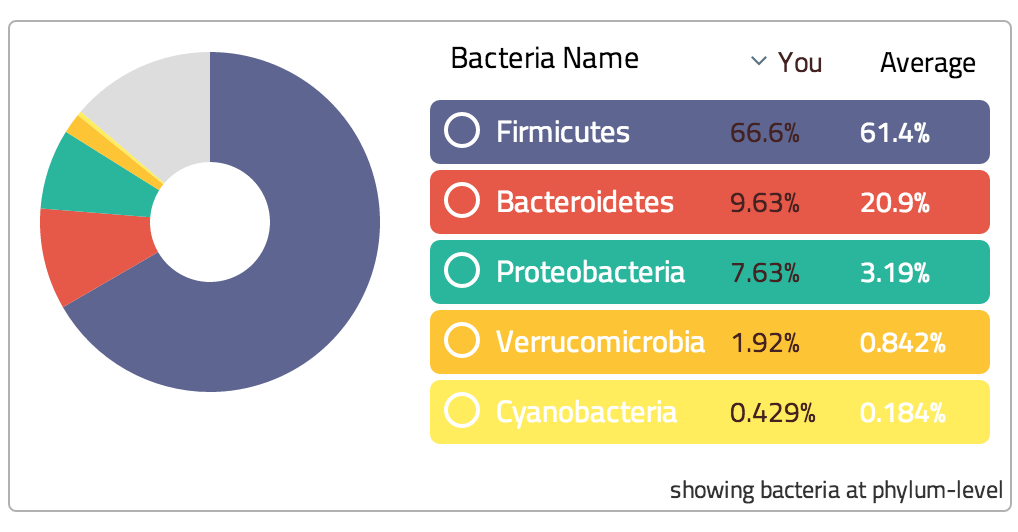
As you can see above, at a phylum level many groups have altered by a factor of 2 from normal healthy people:
- Bacteroidetes are 1/2x
- Proteobacteria, Verrucomicrobia, Cyanobacteria are 2.4x, 2.8x and 2.3x
- For smaller phylums the numbers can be worst, up to a 7x difference.
- Firmicutes are normal ( bifidobacterium and lactobacillus belongs to this family)
Clearly there is a dysfunction of the microbiome. This is not caused by diet, none of the diet groups are anyway close to this distribution. Nor is this causes by antibiotics (which some MDs would claim to dismiss dealing with this shift), uBiome provides a handy table to exclude this speculation.
| Sample Site | Group | Bacteroidetes | |
|---|---|---|---|
|
1
gut |
CFS Patient X | 9.63% | |
|
gut |
Vegetarians | 19.03% | |
|
gut |
Paleo Diet | 20.61% | |
|
gut |
Healthy Omnivores | 20.67% | |
|
gut |
Vegans | 20.91% | |
|
gut |
Heavy Drinkers | 21.89% | |
|
gut |
Weight Loss | 21.17% | |
|
gut |
Weight Gain | 23.08% | |
|
gut |
Antibiotics | 18.31% | |
|
gut |
All Samples | 20.89% | |
Weight
The first item of interest is Bacteroides, which are significant for those CFS that have weight problems. “Bacteroidetes are the most prominent gut microbes in much of the world. They are thought to help protect against obesity because they do not digest fat well….Bacteroidetes are under represented in the guts of Europeans and North Americans” So not only are they low by world standards, they are low by the lowest population! Ok, my audience is brain-fogged so I will not go further into technical analysis but move on to the real concern — treatment! (Assuming that this patient is not vested in CFS and want to move towards remission)
Treatment
We will start with the biggest phylums that have shifts and proceed towards the smaller ones.
Increasing Bacteroidetes
This is a bit of a challenge because normally research is done on how to reduce bacteria (for this family, bad oral members of bacteroidetes). Bacteroides consists of three classes, with the class bacteroidia being the one is measured which breaks down into the following families:
One of the challenges is that most research is centered on killing/decreasing bacteria — not increasing them! I did find a video with suggestions on how to modify it by increasing the intake of polyphenols (for example, Rutin, Quercetin, Ginger ), for example:
- Blueberries
- Wine Vingears
- Fruit
See wikipedia for a list of known foods.
Take
- probiotic Prevotella bryantii 25A [2012] – this is an animal probiotic, may not be available in “human grade”
- Probiotic Lactobacillus casei BL23 [2014]
- Lactobacillus mucosae Dairy Product Culture Collection(DPC 6426) [2014]
- Oligosaccharides 2-fucosyllactose and 3-fucosyllactose [2014] (found in human breast milk). Commercial source may be available soon (article)
- Growth rates on polymerized carbohydrates were as fast or faster than on corresponding simple sugars,” [1990] aka polysaccharides: Chitin(chitosan), Pectins
- Arabionose plays a significant role (gum arabic) 1lb for $19 on Amazon [1990]
Avoidance
- Don’t take rhubarb root (Rheum officinale) [1987]
- Simple Sugars “Growth rates on polymerized carbohydrates were as fast or faster than on corresponding simple sugars,” [1990]
- ALL bacteriocin-producing probiotics know to impact the above, they include:
- Antibiotics:
- metronidazole; imipenem; amoxicillin/clavulanate and clindamycin [2014]
Bottom Line:
The best single item after reading the literature is adding gum arabic to your diet (Recipes: ifood.tv) or make pills of it and take daily (up to 30 gm/day is reported safe! – I would suggest limiting to 8 gm) . There seems to be a significant number of articles on PubMed supporting this suggestion. It is also very affordable! Chicory forage (if available) seems very effective [2014, 2006] as well as high dietary fiber, xylose and non-starch polysaccharides. Tomorrow, I will move on to the next phylum.
As always, this is educational only — any changes of supplements, food, medications should be done in consultation with a knowledgable medical professional.
