My last post deal with microbiome differences seen between healthy individuals and CFSers after stress exercise. In this post I will look at the reported changes (in healthy individuals usually) as a result of exercise in the hope that it may provide hints on what is happening. There was not much. What I found is below.
NOTE THIS MAY OR MAY NOT BE APPLICABLE TO CFS PATIENTS
A 2014 article included the following chart dealing with mice:
- ND – Normal Diet
- HFD – High Fat Diet
- ND+ex — Normal Diet + exercise
- HFD+ex – High Fat Diet + exercise

“Somewhat to our surprise, our data suggest that HFD and exercise independently impact the different behavioral domains of anxiety and cognition, much like the orthogonal effects on the gut microbiome. Though the cognition associations with specific OTUs were weaker compared to anxiety, we nonetheless found significant relationships that all fell within Clostridiales, a diverse taxonomic order within the phyla Firmicutes that has not been previously associated with cognition.. Numerous studies have described how the gut microbiome is altered by a HFD and obesity including changes in Firmicutes and Bacteroidetes [28-31]. Though only a very minor phylum in terms of representation, we also found that HFD reduced the relative abundance of Tenericutes, driven almost entirely by a single OTU (#67) from the genus Anaeroplasma (>99% probability as shown in Additional file 2: Table S2) that has not been previously implicated in dietary manipulations.”
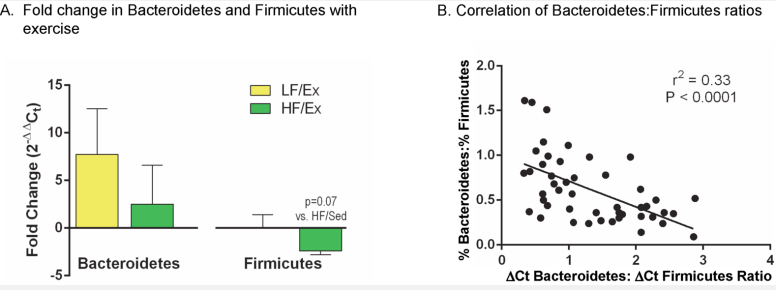
 Another 2014 article looked at mice with Low Fat (LF) and High Fat (HF) diets.
Another 2014 article looked at mice with Low Fat (LF) and High Fat (HF) diets.

“Exercise alters the gut microbiota in mice on both a LF and HF diet and normalizes major phylum-level changes for mice on the HF diet; furthermore, the volume of exercise (total distance run) inversely correlates with the Bacteroidetes:Firmicutes ratio. The Ex-induced gut microbiota in both LF and HF conditions are different than their sedentary counterparts and yet, also different from each other. At the taxonomic level of bacterial family, HF diet induced blooms in some of the major constituent groups within Firmicutes such as Lactobacillaceae, Lachnospiraceae, and Ruminococcaceae and a decrease in the major constituent group of Bacteroidetes, S24-7. Exercise in the HF condition prevented some of the dietary changes, such as with Lactobacillaceae and S24-7, but intensified the blooms seen with HF feeding in others such as with Lachnospiraceae, and Ruminococcaceae. Further exploration of the gut microbiota changes induced by Ex may allow for exploitation of this effect and the development of treatments for obesity and dysbiosis associated with high fat intake.”
From a 2013 article “Diet rapidly and reproducibly alters the human gut microbiome”,
“The animal-based diet increased the abundance of bile-tolerant microorganisms (Alistipes,Bilophila and Bacteroides) and decreased the levels of Firmicutes that metabolize dietary plant polysaccharides (Roseburia, Eubacterium rectale and Ruminococcus bromii). Microbial activity mirrored differences between herbivorous and carnivorous mammals2, reflecting trade-offs between carbohydrate and protein fermentation. Foodborne microbes from both diets transiently colonized the gut, including bacteria, fungi and even viruses. Finally, increases in the abundance and activity of Bilophila wadsworthia on the animal-based diet support a link between dietary fat, bile acids and the outgrowth of microorganisms capable of triggering inflammatory bowel disease”
“Exercise leads to an increase alpha diversity amongst individual’s microbiome, especially the Firmicutes and Clostridiales. Significant differences were seen in commensal bacteria within the phylum, Firmicutes. These included Faecalibacterium prausnitzii, uncharacterized species of genus Oscillospira, Lachnospira, Coprococcus, and uncharacterized families of Clostridiales. These differences in commensal bacteria can lead to healthier individuals more able to fight off certain pathogens. For example, Faecalibacterium prausnitzii is a butyrate producer, which has been shown to be important in maintaining intestinal epithelial health. (Blottere HM et al. 2003) ” [2014 Thesis Paper] – NOTE: Miyarisan is also a butyrate producer which is available as a probiotic and why I suggest it for CFS (there are no studies on its use with CFS — yet).
An interesting 2015 article ,”Leaky intestine and impaired microbiome in an amyotrophic lateral sclerosis mouse model” states: “These changes were associated with a shifted profile of the intestinal microbiome, including reduced levels of Butyrivibrio Fibrisolvens, Escherichia coli, and Fermicus, in G93A mice[Leaky Gut]. The relative abundance of bacteria was shifted in G93A mice compared to wild‐type mice…We observed a reduction in butyrate‐producing bacteria (Butyrivibrio Fibrisolvens). ” – Note: E.Coli is reported to be low or almost non-existent in many CFS patients. Thus Mutaflor (E.Coli Nissle 1917) and Miyarisan (Clostridium butyricum) would appear to be logical probiotics for CFS and IBS (No studies to date on either could be located).
My next post will look at what research has found effective for Leaky Gut
It appears that leaky gut is connected to the low levels of:
- Butyrivibrio Fibrisolvens,
- Escherichia coli, and
- Fermicus
See my next post more in a day or two.