A reader recently asked if CFS patients are immunocompromised. If they are taking no herbs, prescriptions or supplements — then the answer is clear: No, their immune system is generally regarded to be up-regulated, the opposite of immunocompromised. The problem comes when the patient starts to take things to reduce the up-regulation. Then the problem becomes where does the patient ends up. The other side is extremely long term CFS patients that can become immunocompromised because their immune system has become exhausted.
Looking at a TNF-Alpha Suppressor (Infliximab)
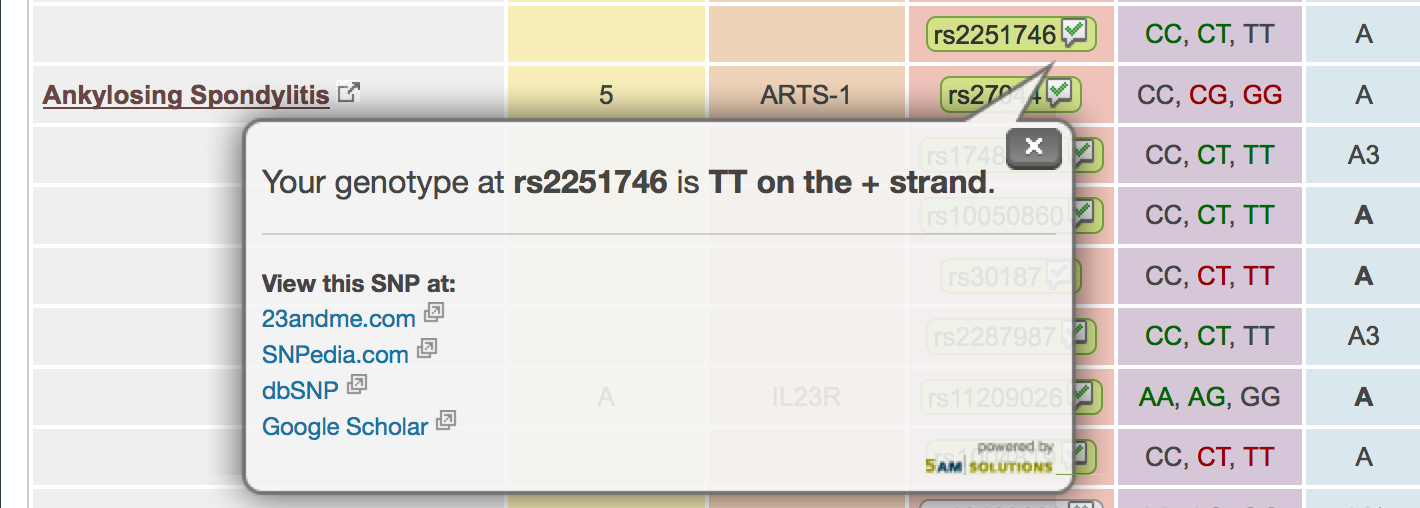
Trying to find literature of immunosuppressing herbs and probiotics is a challenge. In an earlier post, I had given some known TNF-Alpha reducing herbs (Turmeric, Alpha Lipoic Acid, Ashwagandha, Boswellia, Tulsi (Ocimum sanctum) [2014],Neem [many studies]), I am going to drill down on Infliximab, a prescription drug (and “one of the most widely used anti-tumor necrosis factor-α molecules”)
“According to a review of cases of infections caused by bacteria of the genus Lactobacillus from 2005 (collected by J.P. Cannot’a), 1.7% of infections have been linked directly with intensive dairy probiotic consumption by patients.” [2014]
“We describe a case ofLactobacillus bacteremia in a 17-year-old boy with ulcerative colitis managed with systemic corticosteroids and infliximab, who presented with fever to 102°F, flushing, and chills 1 week after starting Lactobacillus rhamnosus GG probiotics. Initial blood culture on day 2 of his fever was positive forLactobacillus, however, subsequent blood cultures on day 3 and 5 were negative. He was treated empirically with antibiotics for 5 days and defervesced by day 8 of his illness. 16 S rRNA sequence analysis identified the organism from the patient’s blood culture and probiotic capsule as L. rhamnosus with a 99.78% match for both the strains. This case report highlights the potential risk of Lactobacillus bacteremia in immunosuppressed patients with severe active ulcerative colitis.” Lactobacillus bacteremia associated with probiotic use in a pediatric patient with ulcerative colitis.[2013]
“Six cases of bacteraemia in hospitalized patients, 5 with a depressed immune status, were caused by lactobacilli. Sodium dodecyl sulfate-polyacrylamide gel electrophoresis of whole-cell proteins and API 50 CH carbohydrate patterns assigned the causative agents to the speciesLactobacillus rhamnosus, Lactobacillus curvatus, Lactobacillus delbrueckii subsp. lactis and Lactobacillus paracasei subsp. paracasei.” –Six cases of Lactobacillus bacteraemia: identification of organisms and antibiotic susceptibility and therapy.[2003]
” a case of meningitis due to Lactobacillus rhamnosus in a child undergoing allogeneic hematopoietic stem cell transplantation” [2010]
” we documented 2 cases of Bifidobacterium longum subspecies infantis bacteremia in newborns receiving probiotics. By comparative genomics, we confirmed that the strains isolated from each patient originated from the probiotics.” Bifidobacterium longum Bacteremia in Preterm Infants Receiving Probiotics.[2015]
“The occurrence of bacteremia with bifidobacteria after its prophylactic administration in VLBW infants” – Case series of Bifidobacterium longum bacteremia in three preterm infants on probiotic therapy. [2015]
There were over 100 articles listed on Pub Med.
Bottom Line
The risk of bacteremia (unhealthy bacteria growth that could be potentially fatal) appears significant if the immune system is suppressed too much either by supplements, drugs or immune-system exhaustion. This is not a total surprise because many of the studies on the health benefits of probiotics were done on “near-normal” populations. There are documented cases for all of the families of bacteria that have been recommended on this site (with the exception of Mutaflor – E.Coli Nissle 1917, and the lack of studies does not imply that it is safe).
This complicated things for long term CFS patients — if you are prone to infections, gum disease, etc then your risk of problems from probiotics are likely higher. Consult with a knowledgeable medical professional (and make sure you quiz them to verify they are knowledgeable and not pompous!).