
A reader wrote today the following
“I know this will and does seem like an excuse to anyone who hasn’t suffered from CFS / Lyme and related illnesses, but I’ve been feeling so depressed and so tired and so dumb the last six plus months that following a complex protocol feels impossible. I don’t know if depression or total lack of motivation is something you’ve dealt with personally, but I would truly appreciate any advice you have. I’m hoping that if I can get some relief in that area that I will feel motivated and less defeated and more clear when trying to start and follow a protocol. “
This is not unfamiliar to people dealing with CFS patients. A lot of the problems stem from the decrease of executive function coupled with difficulty processing information. If you go to any CFS forum, you will hear dozen of opinions often with concerns about taking too much of ABC.
A classic example is concerns about taking above the recommended daily allowance (RDA). The RDA for Vitamin D is 600 IU/day but this level will never result in Vitamin D levels in the body reaching the level that has been shown to reduce symptom severity for Chronic Fatigue Syndrome and Fibromyalgia (prior post). A 2015 study found IBS quality of life improves with increase of Vitamin D. Even Doctor Mercola states “The Institute of Medicine’s (IOM) recommended dietary allowance(RDA) for vitamin D underestimates the need by a factor of 10″ [2015] and recommend 9000 IU. Because of mal-absorption that occurs with CFS, I advocate 15,000 IU. What happens? You walk into your medical professional and tell them you are taking 9000 – 15000 IU/day and they freak out, pressuring you to reduce it to just 600 IU — because that is what is in the official literature.
Most CFS patients ends up having to make their own decisions on what to take and dosages — and with limited cognitive abilities, that is a challenge.
Dealing with Depression
This is a good point to start a list of daily supplements.
- ” evidence of decreased depression risk among women with higher intakes of vitamin B6 from food, which was dependent on total energy intake, and among men with higher intakes of B12 from food” [2015]
- “vitamin B consumption and serum vitamin B12 and folic acid levels were low …among patients with depression.” [2015]
- ” men with deficient vitamin D status were more likely to have current major depressive disorder… Associations among women were not significant” [2015]
So three vitamins should be taken daily
- Vitamin D3: 9000-15000 IU/day
- Folate (B9) – 6,000-13,000 mcg – See this post for studies.
- B12 – 1000 mcg/ 1 mg seems to be the effective ongoing dosage, see this post
- B6 supplementation have been reported to be problematic, I need to do more research
To Avoid: Lactobacillus Acidophilus, a recent study found that higher levels were associated with depression
To Take: See CFS Depression, Diet and the Microbiome
Confusion
Every decision that you must deal with, adds confusion. I have seen patients selecting pills to be exhausting.
One approach that I have done with people that are irregular in taking supplements is to prepare 7 zip-lock bags labelled (Monday, Tuesday, … Sunday). Sorting and selecting pills only need to be done once a week.
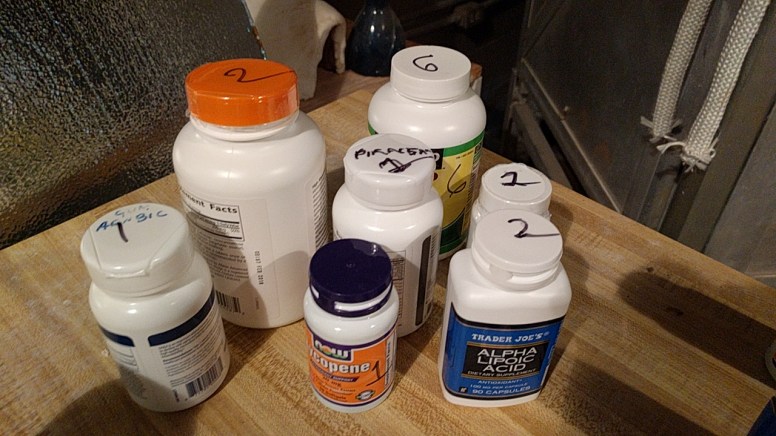
Combining these bags with a marker pen that writes the number of capsules from each bottle (as shown below), eliminates the decisions to be made. For many supplements (except anti-infection ones), keep taking the number specified until the bottle is empty. Many CFSer end up with 1/2 or 3/4 filled bottle of supplements that they stop taking (which does not help a tight budget!). When the bottle is done, consider a different one OR refill OR BOTH!
Fear
Fear is a harder item to deal with. One resolution of not having a cure from the MDs is to simply wait until a cure is found. Will a specific treatment make me worst? An adverse reaction associated to something reported on a forum can result in significant fear about taking something — even when studies have found strong positive effects.
For me, when I was in relapse with CFS, I kept to items with demonstrated positive effects according to PubMed, if some one (even a MD) suggestions something contrary I asked for a pubmed article supporting their belief. If they cannot provide one, then I ignore them — End of influence. Information from forums, while emotionally nice and supportive, are often coming from people with cognitive impairment, poor memory etc etc etc. The information actually comes with significant costs to a CFS patient — a lot of noise that can be very difficult to sort thru.
Where do you go from here?
Three vitamins should decrease depression significantly as well as improve symptoms. If you have been eating yogurt or probiotics high in L. acidophilus, you may wish to stop.
You want to simplify pill taking — do 7 days of pills and do it by only figuring out the dosages ONCE instead of every day.
