Based on several online meeting that I had, I thought a series of online meeting for people to ask questions, be shown features, etc would benefit many.
The meetings are all at 7AM Seattle Time on Saturdays. This should work for most people around the world.
All meetings will be recorded and then posted on YouTube. By attending you consent to being recorded.
I am a statistician and for ME/CFS I took an odds approach to treatment back in 1999. Two treatments reported 90% remission (not improvement) rates from conference reports. They had no apparent connection to each other. I persuaded my MD to do both. Assuming they are not connected much, the statistical odds of remission jumped to 99% doing both. It worked.
I have spent 50 years in Information Technology and tend to use successful patterns from that career. One key pattern is finding isolation points to subdivide the problem (find a wedge point) and then focus on whichever side of the issue it the cause . The other pattern is focus on fixing the problem (often without knowing the real cause of the problem). A file gets corrupted — was it a disk issue, a memory issue, a code defect in the official program using it, a code defect in the libraries (the Operating System’s DNA), a voltage spike, a virus that infected the system (which may have since been removed by an anti-virus update) or human error (from too much booze?!?) in entering or processing the data.
With ME/CFS (and other conditions), many patients and researchers seem to exhibit obsessive compulsive behavior to find the cause; instead of fixing the problem. In some cases, researchers seek fame (or at least more grants) searching for the cause — and likely more publication for their Curriculum Vitae (resume for common people).
Many years ago I started CFSRemission, this blog, with the focus on fixing the problem. Actually problems is a better term because of multiple symptoms. I chose not to work off theories but off clinical studies that improve symptoms (reduce the problem). This makes no assumptions as to the cause.
Request from a Reader
I got this email from a long time correspondent. She has been doing regular microbiome samples (via BiomeSight, discount code: “MICRO”), transferring to my analysis site (Microbiome Prescription) andusing suggestions generated from the microbiome alone (the “Advance Suggestions” mentioned below).
I’m not seeking medical advice but asking how you’d go about things: For years PERSON (CFS) has been following your basic supplement advice as on CFSremission.com, and adding to them your “advance suggestions”. Currently it’s not working for her- though it has in the past, very well! Yesterday her new lab results arrived (Biomesight – thank you very much for easy transference!). Question #1 I’m thinking of abandoning your basic supplements and just using the “advanced suggestions” – is that what you’d do? Or do the lot as long as none of them appear on “decrease”?
Question #2 What’s the relationships between the new “just give me suggestions” and the “advanced suggestions”? Is the latter preferable to follow if we don’t have brain fog? Question #3 To follow Jadin (see this post), do we just pick the two highest rating antibiotics and have them together for 7 days, then in 3 weeks another two antibiotics? That’ll involve that rarity, a compliant doctor! Many thanks,
Answer #1: The material on CFSRemission are from studies — that is group of patients. Typically 80% improve 10% has no effect and 10% get worse. The group as a whole improved. This does not mean an individual will. To return to the odds motif, if you do enough of them, the odds are that you will improve. It is very similar to picking stocks — some will go up in value and some may go down… there is a little gamble involved.
In recent years, there have been more and more studies showing that the effectiveness of treatment (even for cancer) depends on the microbiome. In keeping with stacking the odds in favor of the patient, I would go with suggestions from the microbiome analysis that are also shown to help ME/CFS. You want two check marks!
The second aspect is resistance. There are many ways an infection or other “source” will survive and subsequently flourish. Whatever works today, may fail tomorrow. Back to my usual work environment, the next mutation of a computer virus may not be stopped by your antivirus software. The next infection may not come from the internet but from someone plugging in a USB drive. It may come embedded in the official release of a computer application. The human system is a lot more complex than any computer system. Many people view it as a static system made up of Lego blocks; it is far closer to a herb garden containing dozens of herbs and fruit trees. People grossly underestimate this complex system agility to adapt and evolve.
The need for regular rotation of all modifiers/substances has been growing in my understanding. The original concept came from Cecile Jadin and applied to antibiotics. Subsequently I found published studies confirming this approach produced better results. This was then extended to probiotics because they produce natural antibiotics. This was then extended to antibacterial and antiviral herbs and spices. All for the same reason, bacteria and virus adapt. The last step, rotating everything — including vitamins — is now in my suggested approach stated in the new PDFs New Reports for Medical Professionals.
Last week I was discussing this with a recently minted doctor, Chidozie Ojobor, Ph.D. who’s thesis was in this area and he was in complete agreement.
The recommended process to obtain a persistent shift of the microbiome is: * Generate 4 lists from the suggestions with nothing repeated on another list * Emphasize one list each week * After 8 weeks (2 cycles), retest the microbiome to obtains the next set of course corrections This approach allows the microbiome to stabilize towards normal.
Answer #2: The “just give me suggestions”, on Microbiome Prescription, is intended for the technically, biologically, and medically challenge. Often these people have brain fog or other neurological challenges. Its intent is to give suggestions with good odds. Advance suggestions is the person that wants to “hack themselves”. It presents a literal smorgasbord of different approaches (whatever people asked for has been tossed into it); I have also include some of my experimental approaches (especially around KEGG derived data). Adding in the consensus feature — where you can try dozen of different approaches and see what most of the approaches agree on — is a subtle attempt to stack the end-suggestions towards good suggestions (without being dogmatic).
One of the features of the advance suggestions is this: I have 6 conditions listed on the Medical Conditions with Microbiome Shifts from US National Library of Medicine page and three symptoms on Special Studies Suggestions. I want to know what I can take that is likely to help all of these. You can do each and then get your answer from the consensus page. If you have done two different labs at the same time, you can then do the Uber Consensus located on the Multiple Sample pages. The results are highly probable suggestions without debating which lab is better.
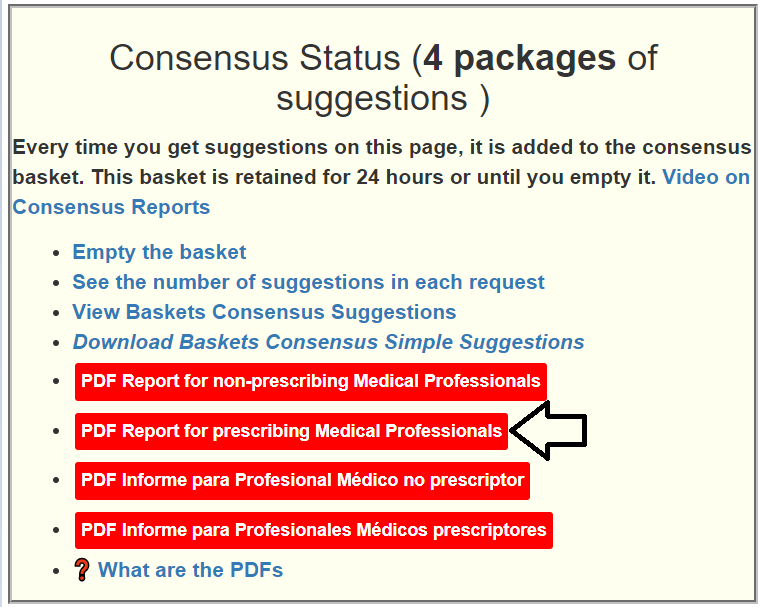
Answer #3: If you go to the Changing Microbiome tab, you will see 4 red buttons
Clicking the prescribing Medical Professional one will generate a report containing antibiotics often. Below is the latest for the person you referred to. There are 4 listed. Those are the ones that likely have the best odd — favored to correct the microbiome and also favored by Dr. Jadin (see Dr. Jadin’s Current Protocol for ME/CFS)
Beware of Social Influencers!
People saying “it worked for me” or “This is what ME/CFS is and thus this is how you should treat it” are the biggest threats to successful treatment. The microbiome influences almost every medical condition and appears to be very connected to symptoms and speed of progression. It may not be the cause — it is likely a “chicken and the egg” question (which came first); or in more computer terms, it’s a feedback loop that needs to be broken. The microbiome is a far easier target than whatever is “behind door #2”.
My answer is simple: Yes — but the mechanism may be one of several possible. The most likely are:
Environmental influences.
Family behavior patterns (i.e. stress level run high)
Explicit DNA Mutations
Shared microbiome signatures
Despite a prevalence of ∼0.2-0.4% and its high public health burden, and evidence that it has a heritable component, ME/CFS has not yet benefited from the advances in technology and analytical tools that have improved our understanding of many other complex diseases.
Some paediatricians will have noted a family history of CFS/ME and may have wondered whether this was due to genetic heritability or an environmental factor.
A heritable component is implicated by the reported increased risk in relatives of ME/CFS patients [10,11,12], and genetic association studies are emerging in order to identify risk variants. We have recently reported associations with specific HLA alleles, HLA-C*07:04 and HLA-DQB1*03:03 [13], and individuals carrying either one or both risk alleles seem to more often respond positively to the immunosuppressive drug cyclophosphamide [14]
A simple example is a house with a mold issue. The parents may be impacted by the mold, and it is likely that the children will also be impacted. Recently I saw that mites (Chiggers) can spread disease causing bacteria. If one in the household has an asymptomatic infection, it may well spread to others in the family. The household may live in an area where there is pesticide drift. The sensitivity to these factors may be genetic or epigenetic. An environment factor that pre-dispose one child to ME/CFS will likely influence other children of the same family.
“Research to date has demonstrated the initiation of neurobehavioral sensitization by volatile organic compounds and pesticides in animals, as well as sensitizability of cardiovascular parameters, beta-endorphin levels, resting EEG alpha-wave activity, and divided-attention task performance in persons “
This actually has at least two subsets. Defects causing hypercoagulation and general ME/CFS ME/CFS population is the one that I am more, if too familiar with. The general population is prone to a large amount of noise and typical finding is that a third or less of ME/CFS patients have a relevant mutation, while the same mutation is seen only half as often in the general population. This means that 2/3 of ME/CFS patients will not have this mutation – so limited value for making a diagnosis. If you have a specific mutation that is known to be treatable, then that should be factored in.
The hypercoagulation SNP is different because you are not looking for a mutation shared by all ME/CFS patients but mutations already known to encourage coagulation. Dave Berg pioneered this work.
Bacteria may be transferred by a kiss or even touching. Similar diets will encourage the same profiles. Like the environment, it may pre-dispose people in the same family because of the shared food, and the shared microbiome.
With this less documented dimension, the microbiome may be pre-disposed towards being dysfunctional. Similarly, the microbiome may pre-dispose a person to have high anxiety. Things become a bit more complicated because the microbiome is influence by DNA (and the reverse). There was a Chinese study that I remember reading where both COVID severity and Long COVID was associated with people’s pre-COVID microbiome (they happen to have been running a large time-lapse study on the microbiome)
Bottom Line: It does run in Families
My suggestion for action plans for those concerned:
Improve the environment as much as is possible.
Reduce the exposure to pesticides and man-made chemicals (for example fragrances). It is very common for ME/CFS people to develop acute sensitivity to many chemicals which hints that they may be a contributor to the condition.
Check for molds and fungi. Monitor the humidity levels in your living space and take action as needed
If type-A personality or high anxiety is a factor, learning better coping mechanisms or lowering expectations may help. Do set expectations on other people!
Microbiome Analysis and changing diet to better normalize. The microbiome appears to influence anxiety greatly. Also Gut bacteria linked to personality[2020]
DNA testing — technically it could help, but still early days for research. The one exception is testing for inherited genetic coagulation factors.
Needless to say, I favor microbiome manipulation greatly — because it is the easiest factor to address (can be hard to give up favorite unhealthy foods).
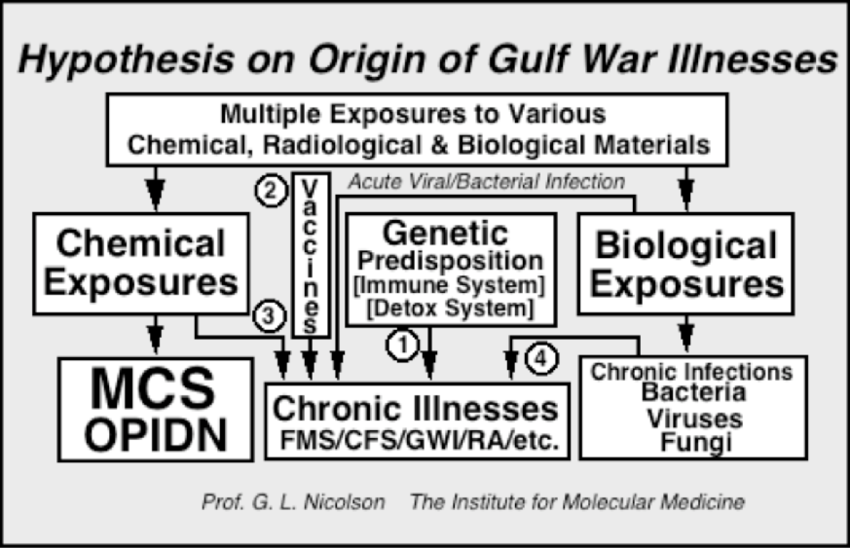
Back in 1990, Garth Nicolson believed that mycoplasma was the cause of both. I actually appear on a news report with him as a sample patient doing antibiotics (but different ones). Some of his articles:
1998, Diagnosis and Treatment of Chronic Mycoplasmal Infections in Fibromyalgia and Chronic Fatigue Syndromes: Relationship to Gulf War Illness[5]
2004, Review – Gulf War Veterans: Evidence for Chromosome Alterations and Their Significance[11](Abstract)
2006, Lipid Replacement and Antioxidant Nutritional Therapy for Restoring Mitochondrial Function and Reducing Fatigue in Chronic Fatigue Syndrome and Other Fatiguing Illnesses[12](Abstract)
2014, Lipid Replacement Therapy: a natural medicine approach to replacing damaged lipids in cellular membranes and organelles and restoring function.[14](Full Text)
2014, Mitochondrial Dysfunction and Chronic Disease: Treatment With Natural Supplements.[15](Full Text)
2017, Membrane Lipid Replacement for chronic illnesses, aging and cancer using oral glycerolphospholipid formulations with fructooligosaccharides to restore phospholipid function in cellular membranes, organelles, cells and tissues[16](Full text)
“WASHINGTON, D.C.–A major trial has found no evidence that antibiotics help patients with Gulf War illness. Moreover, the outcomes of the $6 million study suggest that the hypothesis underlying it–that a microbe causes the mysterious set of complaints–is false.”
Back in 1999 when I had major ME/CFS, Nicholson’s protocol was one that I considered but did not take because I perceived Jadin’s Protocol to be significantly better [ Dr. Jadin’s Current Protocol for ME/CFS ]. I knew enough about antibiotic resistance to deem any monotonic(just one) antibiotic (or that matter, anti-viral) protocol to likely fail over time. The classic model of antibiotics is that it reduces the infection to the point that the body can take over bacteria suppression. If the immune system is misfiring, this becomes a major and wrong assumption.
Since those days, my understanding is that the cause of ME/CFS, Chronic Lyme and Q-Fever, and Long COVID is not a single bacteria (or virus) infection. It is an altered microbiome placed into a dysfunctional state by a bacteria, infection, stress or other environmental factor; and the microbiome was unable to return to normal. It is unlikely that a single antibiotic taken continuously will remedy this situation. Normalizing the microbiome is a complex thing and, IMHO, requires continuous intelligence (i.e. microbiome tests).
With the Remission Biome Project for ME/CFS we are seeing subject and objective (i.e. in follow-up microbiome tests) improvements.
For more information on this project see Health Rising post. Both participants has granted me to do a review with their real names. This is the second of a series of posts on this project, the first one was on Tess Falor.
The earliest use of antibiotics for treating ME/CFS that I am aware of, dates from the late 1990’s with articles in Journal of Chronic Fatigue Syndrome (and conference reports prior)
My remission from ME/CFS was done by combining C.L. Jadin protocol with Dave Berg anticoagulant protocol.
A big thanks to BiomeSight.com for donating some testing kits to the project. If interested in using their kits, there is a discount code (“micro”). For another person in this project: The Remission Biome Project: Tess Falor
Overview of results
First, let us show the numbers and then talk about them. It is clear that there are significant changes. There are a lot of dimensions to consider. Some highlights:
The number of bacteria with abnormally high representation has gone from 123 down to 29
The number of bacteria with abnormally low representation has gone from 222, dropping down to as low as 19, before rebounding to 162 (still better than the start)
Most measure showed great improvement and then some relapse.
Criteria
7-Mar
23-Mar
15-Apr
22-Apr
29-Apr
Shannon Diversity Index
33.8
78.0
97.1
76.5
77.1
Simpson Diversity Index
0.7
65.1
58.6
60.3
73.4
Chao1 Index
91.3
61.6
72.0
89.4
14.8
Chi-Square (Lower is better)
55
47
46
50
30
Lab Read Quality
8.6
7.1
5.4
2.2
6.9
Bacteria Reported By Lab
755
638
628
765
461
Bacteria Over 99%ile
27
11
13
56
5
Bacteria Over 95%ile
72
25
30
105
18
Bacteria Over 90%ile
132
46
63
178
29
Bacteria Under 10%ile
222
218
62
19
162
Bacteria Under 5%ile
191
195
18
12
144
Bacteria Under 1%ile
177
179
0
3
112
Lab: BiomeSight
Rarely Seen 1%
8
4
3
66
2
Rarely Seen 5%
22
24
27
128
14
Pathogens
39
32
33
31
29
Outside Range from JasonH
8
8
8
8
8
Outside Range from Medivere
18
18
16
16
16
Outside Range from Metagenomics
9
9
6
6
6
Outside Range from MyBioma
10
10
6
6
6
Outside Range from Nirvana/CosmosId
18
18
12
12
12
Outside Range from XenoGene
52
52
39
39
39
Outside Lab Range (+/- 1.96SD)
43
15
17
36
7
Outside Box-Plot-Whiskers
146
51
83
227
43
Outside Kaltoft-Moldrup
251
189
105
212
158
Condition Est. Over 99%ile
1
5
0
0
3
Condition Est. Over 95%ile
2
14
0
5
13
Condition Est. Over 90%ile
11
28
2
11
21
Enzymes Over 99%ile
7
68
5
19
37
Enzymes Over 95%ile
22
281
209
123
250
Enzymes Over 90%ile
58
435
361
317
409
Enzymes Under 10%ile
219
354
59
48
201
Enzymes Under 5%ile
173
265
34
24
144
Enzymes Under 1%ile
138
94
13
12
79
Compounds Over 99%ile
3
44
1
13
16
Compounds Over 95%ile
15
186
82
68
87
Compounds Over 90%ile
27
297
154
153
183
Compounds Under 10%ile
882
889
985
987
875
Compounds Under 5%ile
862
859
959
963
841
Compounds Under 1%ile
845
802
935
952
820
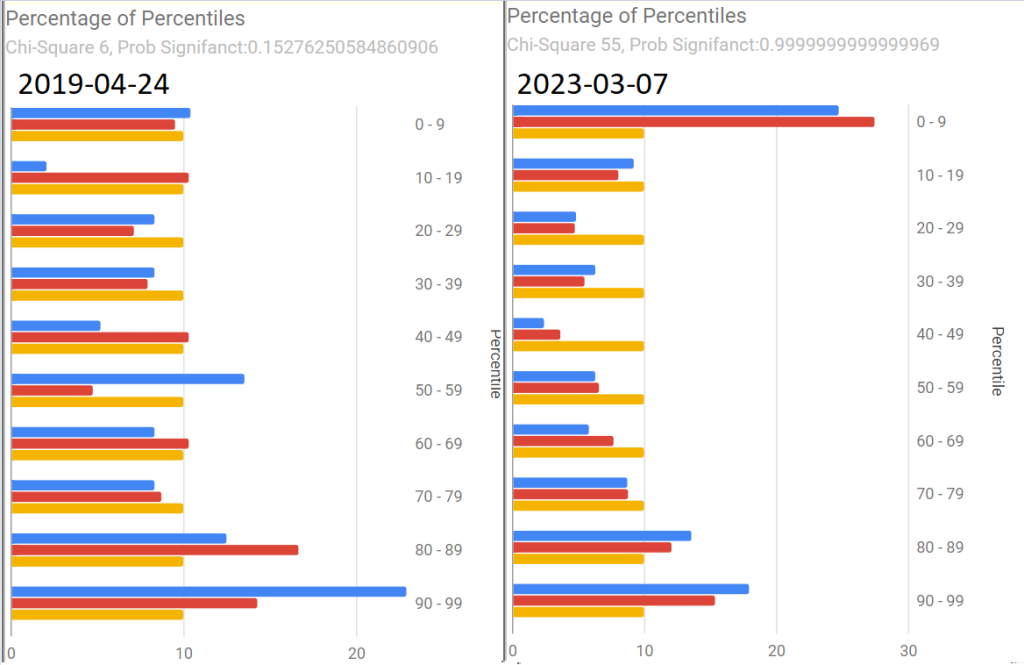
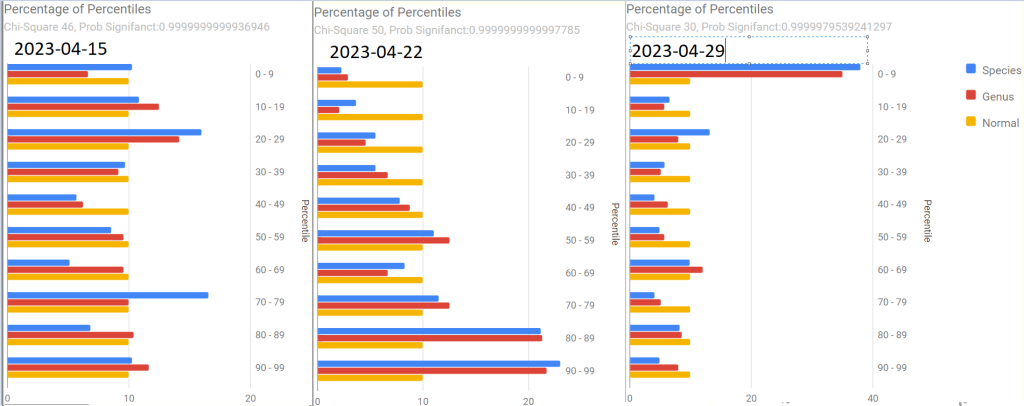
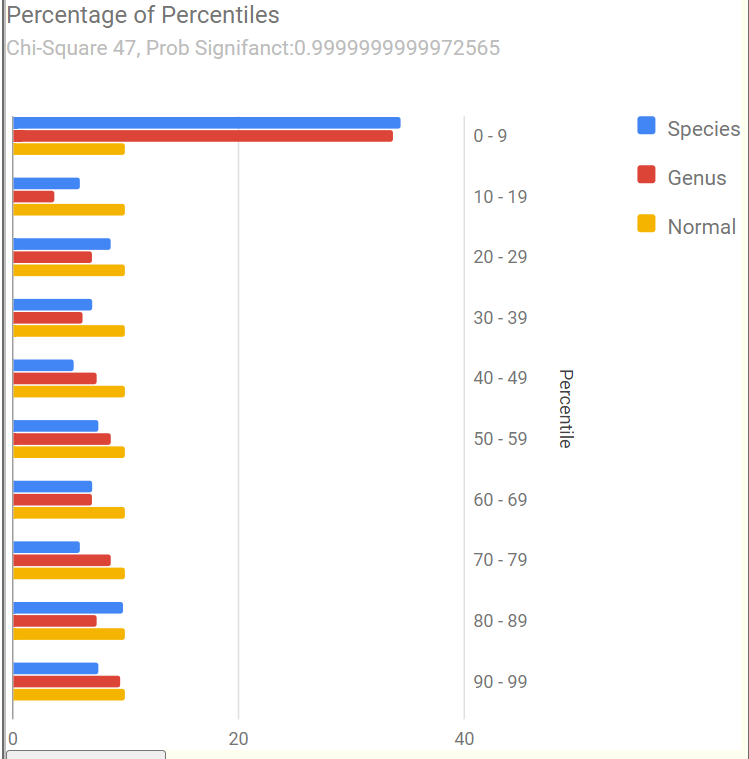
As with Tess, the percentages by percentile which I noticed tend to have over representation with ME/CFS and Long COVID in the 0-9 percentile. We see this pattern at the start, with improvement and then a bounce back to high numbers in the last sample
Tamara suggested that I convert the tables below to charts. Both are now available on the site.
Pretty Pictures
Tamara suggested that I convert the tables below to charts. Both are now available on the site.
First, an old sample that she happened to have where we see Chi-Square at 6. The first of the recent samples had it jumping to 55, A normal microbiome is expected to have a Chi-square < 13. A higher value indicates a statistically significant, abnormal microbiome.
The next three show the changes with antibiotics. Chi-square went from 46 to 50 with a dramatic shift and then drifted down to 30.
The latest sample increased upward again, with the pronounced spikes that are common with ME/CFS being there.
The raw numbers are also shown. I will spare your eyes by omitting them.
The Events Around the above Samples
7 Mar – Before
23 Mar – Day 4 AmoxClav
15 Apr – More
22 Apr – Final Day of AmoxClav (30 days of AC)
This sample has a low Lab Read Quality, this may account for the number of spikes in its report.
29 April – After 3 days of Aprepitant + Erythromycin (this was a BIG difference from Tess and was the intervention that seemed to give me the baseline increase this time).
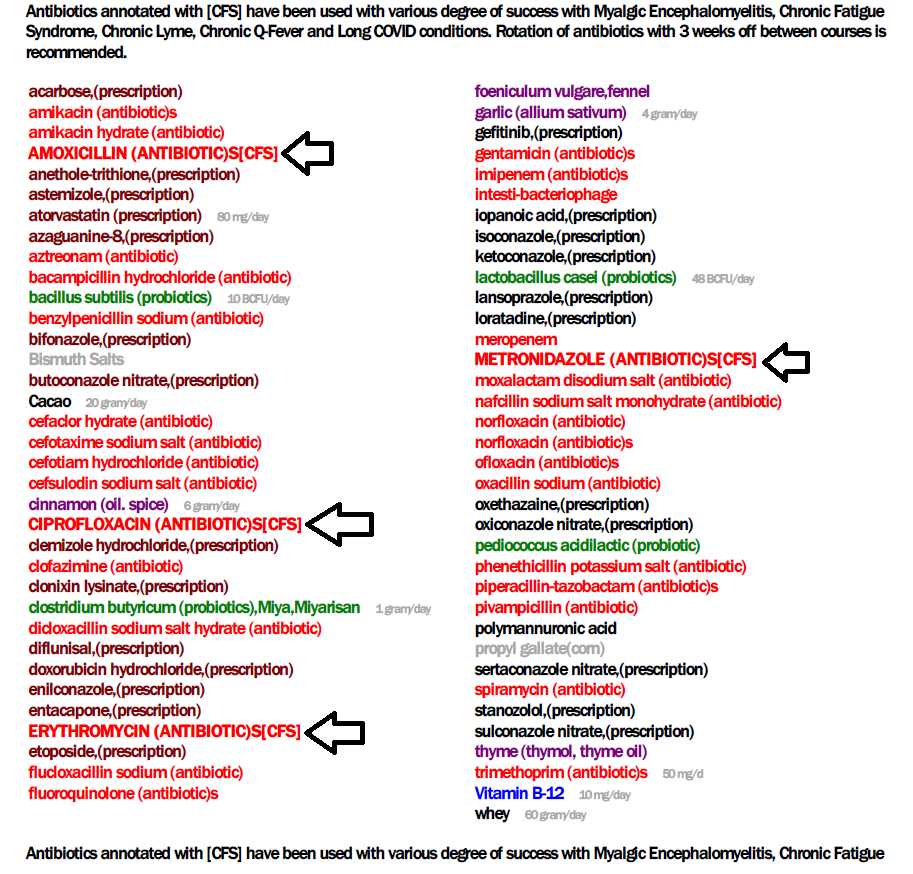
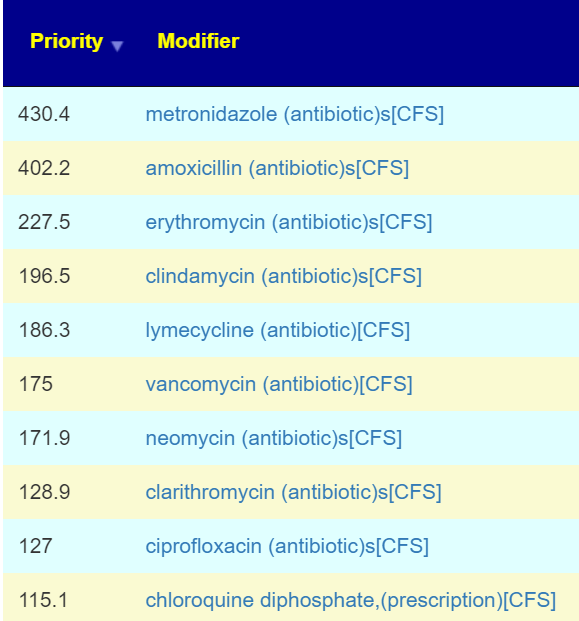
As with Tess, let us see how these items rank in each sample. As with Tess, imipenem is the most common best suggestion.
As a result of a conference call with some of the Remission Biome Project, and Dr. Jadin’s Current Protocol for ME/CFS. I annotated all of the antibiotics used in studies for ME/CFS, Lyme, and related conditions with [CFS]. This allows us to quickly see the “consensus” antibiotics (i.e. used in studies and suggested by microbiome prescription algorithms).
The top ones are shown before (Just enter “CFS” in the Search dialog)
Only two of these were negative for her (doxycycline and ampicillin) with docycline sibling, minocycline being just 21).
I would suggest using this list to pick 2 antibiotics to do a one week course and then take a 3 week break. After the course, then do some of these probiotics. I am inclined to omit L.Casei because the strain used in Yakult is a negative. Thus we end up with these three as top suggestions. P.S.
Note the weight of these are above many of the antibiotics above. I usually advocate single species. The Bifido is available from Custom Probiotics with their recommended dosages above the amount listed above.
Part Deux — More Samples!
Her description of subjective changes: generally keep improving in terms of PEM, function etc. (was definitely a dip around the 2nd ‘constipation’ sample)
1st, [2023-06-14] in the series just a temporal sample, no additional treatments
2nd, [2023-07-15] in the series I had a major episode of constipation – wanted to catch that
3rd, [2023-07-20]last one was was post my 2nd treatment of aprepitant+erythromycin
Sample Comparison
We include the prior one above for easy reference). The key change items are:
The new Anti inflammatory Bacteria Score has seen a dramatic increase from 17%ile to 73%ile. The four prior samples were 7.6%ile, 8.2%ile, 3.9%ile and 6.9%ile
Outside Kaltoft-Moldrup is dropping. In terms of %age of reported: 32% -> 28% -> 29% ->16%
The high and low Enzymes also seem to be dropping
The last sample had a Chi-Square of 9, that is a probability of 0.54 instead of the .9999999… for all other samples. Unfortunately, the poor read quality makes this fuzzy.
Note: The last sample has a low read quality (thus less bacteria types are being reported)
Criteria
22-May
14-Jun
15-Jul
22-Jul
Shannon Diversity Index
69.4
29.20
43.00
15.00
Simpson Diversity Index
54.7
7.60
27.50
60.00
Chao1 Index
72.4
0.87
21.40
8.30
Anti inflammatory Bacteria Score
17.0
30.90
43.60
73.20
Chi-Square Score
49
51
32
9
Lab Read Quality
7.2
10.9
6.6
2.3
Bacteria Reported By Lab
659
752
512
375
Bacteria Over 99%ile
10
12
1
4
Bacteria Over 95%ile
22
24
2
20
Bacteria Over 90%ile
45
41
13
39
Bacteria Under 10%ile
199
229
189
19
Bacteria Under 5%ile
186
208
184
3
Bacteria Under 1%ile
167
165
166
0
Lab: BiomeSight
Rarely Seen 1%
25
13
0
0
Rarely Seen 5%
49
37
7
1
Pathogens
32
34
36
21
Outside Range from JasonH
4
7
7
4
Outside Range from Medivere
14
19
19
14
Outside Range from Metagenomics
6
7
7
6
Outside Range from MyBioma
4
6
6
4
Outside Range from Nirvana/CosmosId
18
19
19
18
Outside Range from XenoGene
33
34
34
33
Outside Lab Range (+/- 1.96SD)
11
12
1
13
Outside Box-Plot-Whiskers
56
75
23
50
Outside Kaltoft-Moldrup
209
212
150
61
Condition Est. Over 99%ile
0
0
1
0
Condition Est. Over 95%ile
0
0
1
0
Condition Est. Over 90%ile
1
0
3
0
Enzymes Over 99%ile
62
1
5
2
Enzymes Over 95%ile
130
3
18
11
Enzymes Over 90%ile
215
12
99
33
Enzymes Under 10%ile
429
211
171
304
Enzymes Under 5%ile
310
146
142
211
Enzymes Under 1%ile
152
85
73
47
Compounds Over 99%ile
31
0
3
1
Compounds Over 95%ile
64
2
9
11
Compounds Over 90%ile
106
7
48
24
Compounds Under 10%ile
959
1096
1009
1015
Compounds Under 5%ile
909
1041
981
971
Compounds Under 1%ile
860
1009
956
922
Since we had a symptom of constipation, let us see how well the samples match that reported from Studies on PubMed — there were no matched. When we went to our Special Studies, we see that the microbiome followed the reported symptoms. We then look at the top value from Special Studies — which was Long COVID for all samples. We see the lost of ground around the constipation and then regaining the progress.
Criteria
22-May
14-Jun
15-Jul
22-Jul
Special Studies
7%ile
14%ile
15%ile
7%ile
Top Item Long COVID
35 %
44 %
41 %
36 %
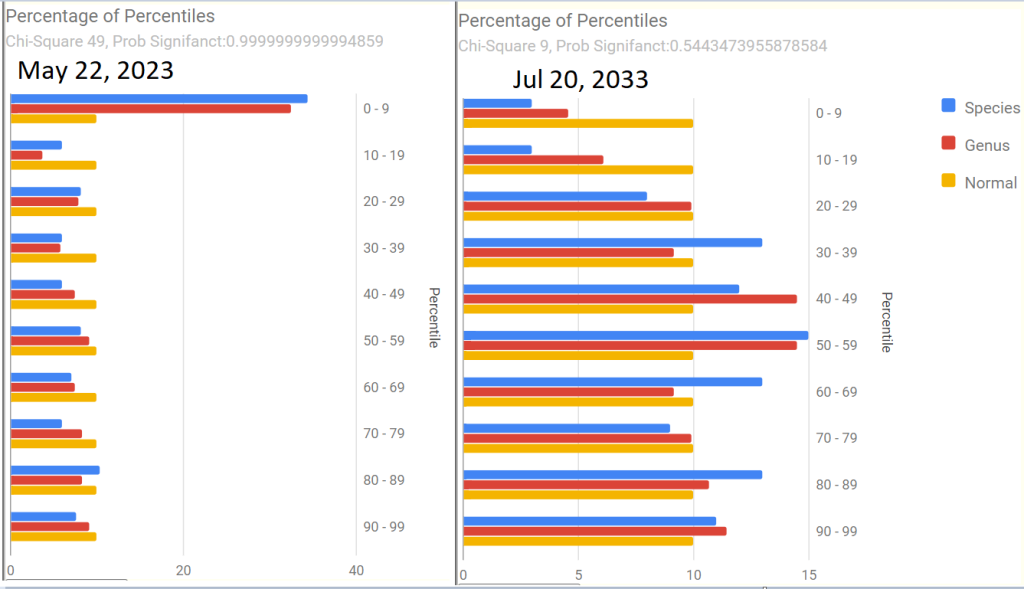
Next we go and look at aprepitant and erythromycin
The Percentage of Percentile show quite a shift — unfortunately, it is unclear if this is a temporary after effect of constipation, poor lab read quality, or the above aprepitant and erythromycin. The next sample may resolve this issue.
Is the Project working — YES
We are seeing both subjective improvement and object improvements.
Personally, I like what appears to be a shift towards Cecile Jadin’s approach — not continuous antibiotics but a course (7-10 days) followed by a break (ideally 3 weeks). Often I find that ME/CFS people tend to be impatient and just want to keep pressing on hard… which I have observed often result in tripping and rolling down the hill to where they were (or worst).
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide information on rotations etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.