Cécile Jadin, MD, has very graciously put together a power point on the state of her protocol and allowed me to share it. This protocol has been in use for over 25 years by her with a high success rate (90%). The protocol actually dates back around 50+ years (for a condition with a different name).
For earlier notes from her, see C.Jadin Resources which links to some of her earlier presentations.
My Experience
The basics of this protocol put me into remission around 2000 and has put me into remission for flares. Far more important, it resulted in my understanding the complexity of this condition’s treatment. Even today, I view many MDs keeping to a naïve one-shot magic-bullet approach: “we need to find the virus (i.e. EBV, HHV6, etc) or bacteria that triggered it; find a drug to treat it and the patient is cured!” I have read so many accounts of people being “cured by X, but it stopped working after N months and X does not work anymore”.
Dr. Jadin has many decades of clinical experience treating ME/CFS and related conditions. She built upon clinical experience treating this type of condition. I have decades of doing software development.
Jadin and I are two sides of a Treatment Coin
Cécile Jadin is a MD with decades of clinical experience treating ME/CFS applying and evolving a protocol that she inherited from her father’s time at the Pasteur Institute of Tropical Medicine. I am a high functioning autism person well trained in Artificial Intelligence and Statistics who has applied it to the microbiome. My AI algorithm very very often suggests the same set of antibiotics and supplements that she uses. The algorithm works off bacteria only (and thus ignores many other co-factors). We walk different paths and end up in the same treatment approach.
She talks about Obligated Intracellular Organism or OIO. This term may be unfamiliar to many, for some background readings see this Research Topic on Frontiers. I talk about the bacteria in the gut.
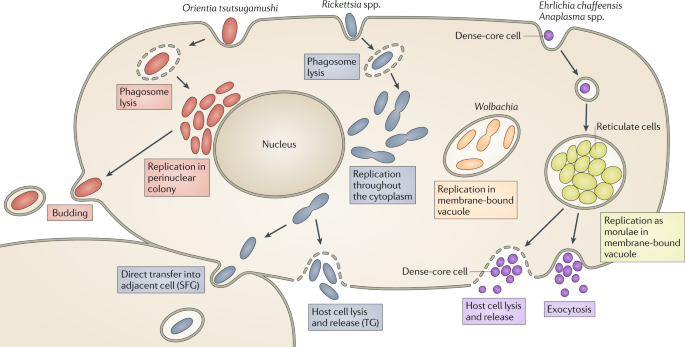
From: Cells within cells: Rickettsiales and the obligate intracellular bacterial lifestyle [2021]
They are very interconnected with a lot of information exchanged between them. OIO sends mis-information messages to the gut to produce more of this or that enzyme, metabolites, compounds [Products]. There are over 26,000 different products potentially involved. The gut receives this information and fill these bogus orders. The OIO gets its supplies and proceed to prosper. A side effect of these bogus production orders are symptoms – they could be view as pollution from the production. The symptoms often depends on a person’s DNA.
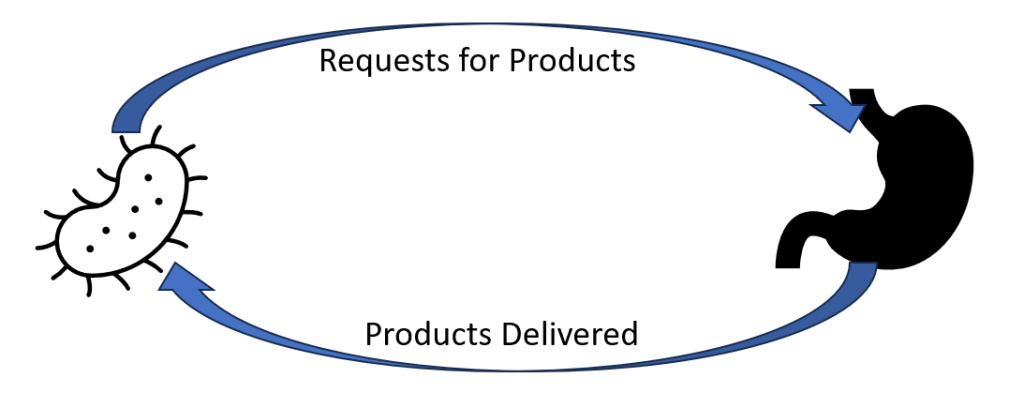
This cycle needs to be broken. This may be done by attacking the command center (the OIO) or attacking the factories (the microbiome) or both.
Original Motivation
One of the goal of building my AI was to try to identify the factors for non-responders. To me, it appears to be due to variations in the microbiome. Recently there has been many studies reporting that the difference between responders and non-responders for both cancer treatment and the severity of COVID has been the patients microbiome. The AI can suggest what to take; Jadin’s clinical experience provides information on how to take it.
Remission is the Target, not who is right
Patients and their MDs can go down two path, the paths actually run besides each other.
- Follow Cécile Jadin process and protocol precisely
- Follow Cécile Jadin process but use iterative sets of suggestions from Microbiome Prescription. By that, pick 1-2 of the top CFS tagged antibiotics, then at the end of first month, take a new microbiome sample and start with the secondary CFS tagged antibiotics (while waiting for the results).
- See this post for the suggested cycle.
The latter approach can be tried without prescription antibiotics because it identifies probiotics (that often produces natural antibiotics) and herbs (with antibiotic characteristics) and thus allows self-treatment for those without a cooperative medical professional. This no-antibiotics approach will likely work slower for most people. I discourage self-treatment, but often there is no alternative. My first choice is keeping strictly to clinical experience using the microbiome suggestions to select between clinical alternatives.
The Cécile Jadin’s process of alternating substances with breaks is a critical factor. In terms of modelling effectiveness (my expertise) — there is no question, it is the rational approach that treats everything as living entities and not mechanical nuts and bolts.
Video Presentation by Cécile Jadin
Short Version (35 minutes)
The bare presentation.
Long Version (65 minutes)
This version includes questions and answers from participants(and chit-chat). Her presentation starts at 5 minutes into it. At the end a patient shares her experience after the first 3 months.
Power Point as a PDF
You may download her presentation below as a PDF file. Or listen to it on YouTube which is intended for people having difficulty reading (common symptom with ME/CFS).
Treatment Fundamentals
Antibiotics (with alternative names) and links to known microbiome impact and alternative names where available.
- Doxycyl 100mg x 2/day + Ciprofloxacine 500 mg x 2/day x7 days– No exercise!
- Lymecycline 300mg x 2/day x 7 + Metronidazole 400mg x 2/day x 7 days – No alcohol!
- Minomycine 100mg x 2/day x 7 + Rulide 150 mg x 2/day x 7 days
- Doxycyl 100 mg x 2/day + Tavanic 250mg x 2/day x 7 days– No exercise!
- doxycycline
- levaquin (no info)
- Clacid 500mg x 2/day x 7 + Augmentin 1.000 mg x 2/day x 7
- clarithromycin
- amoxicillin
- clavulanic acid – no info
- Dalacin C150 mg 2 x2/ day x 7 days – Given alone for best results
- Doxycyl 100 mg x 2/day + Avelon 400mg x 2/day x 7 days– No exercise!
- doxycycline
- avelox – no info
- Tetralysal 400mg x 2/day + Dapsone 100mg nocte (stop if blue lips) x7 days
- lymecycline (variation)
- dapsone
- Vibramycine 100mg x 3/day x 7 days – Given alone for best results
- doxycycline (variation)
- Nivaquine
“All those antibiotics MUST be taken: after food ( not only water ) and without any dairy products. Patients must avoid sugar intake and some supplements(for example magnesium, glutamate, vitamin D). Antibiotics should be taken in the morning and the evening”
“Duration of treatment: 1 – 3 years.” Symptom remission may occur sooner, but that is usually just a tactical victory and not a strategic victory. You won one battle, but the war is not over.
Probiotics:
“Taken at noon only. No specific ones, but they must also be rotated (like the antibiotics)”
The Testing Dilemma
Dr. Jadin pointed out there are no testing facilities for some types of OIO in the US, Australia or Europe. When patients samples are sent from these “OIO free zones” to labs that test for them, often the results come back positive. Today everyone knows about invasive species (ticks, plants etc) but frequently ignore biological human invasive species. A few are known: smallpox, polio and a small number of others are associated with travellers. These are old diseases that were known and eliminated. Tourists often pick up unfamiliar diseases that their personal physicians know nothing about: Ascariasis (hookworm), Buruli ulcer (Mycobacterium ulcerans infection), Chagas disease (also known as American trypanosomiasis), Dracunculiasis (Guinea-worm disease), , Trypanosomiasis, human African (sleeping sickness), Leishmaniasis, Leprosy, lymphatic filariasis, Onchocerciasis (River blindness), Schistosomiasis, Trachoma (Chlamydia trachomatis), and Trichuriasis (whipworm).
Many of these conditions can be transferred from human to human with someone who has never been to Africa having an OIO and those can be unknown in your country (without lab test facilities being available) but they are well known in Africa or South America. You may be told: “So, we have run tests for everything and everything came back negative — you have an atypical condition with no known treatment”.
Bottom Line
Medical treatment suffers from one dimensional linear thinking that often uses a “nuts and bolts” mechanical model. The model and understanding of Dr. Jadin assumes a living organization that changes and adapts. The problem bacteria (be it OIO or microbiome) will literally play hide and seek with treatments. I share this perspective.
Some Possible Paths Forward
Depending on the cooperation of your MD, availability of detailed microbiome tests, etc.
- Follow Dr. Jadin protocol
- Follow the path being discussed in the Remission Biome Project:
- Using Microbiome Prescription to generate a list of candidate antibiotics and then take the highest ranked on that which is on Dr. Jadin’s list – following Dr. Jadin’s pattern of alternating and pulsing
- Implement the non-prescription suggestions of to avoid or to take. That targets the factory side (that is the gut microbiome), not the OIO side of the cycle show above. It simply improves the odds.
- Do not use antibiotics (either by choice or by lack of cooperating MD) and use the advanced suggestions based on your microbiome sample with a new microbiome test every 6-8 weeks. Each new test will alter suggestions (especially probiotics). All suggestions should be reviewed by your medical professional.
See this post: We can suggest what to take, but not how to take! for a more explicit description.
Follow Cécile Jadin process but use iterative sets of suggestions from Microbiome Prescription. By that, pick 1-2 of the top CFS tagged antibiotics, then at the end of first month, take a new microbiome sample and start with the secondary CFS tagged antibiotics (while waiting for the results).
- See this post for the suggested cycle.
A quick apparent remission may occur after the first antibiotic, Dr. Jadin’s opinion is that you need to keep to it for at least a year, in some cases up to 3 years. Having a remission that lasts 3 months and then relapses makes the next remission much harder to obtain.
A current project using antibiotics has two analysis done showing significant subjective and objective improvement.
Questions and Answers
Q: “This doesn’t address the causes of ME/CFS. Also there’s no mention of any nutrient deficiencies typically seen in every case of ME/CFS I’ve seen, or genetic factors, or anaemia, or thyroid dysfunctions, or other causes and factors.”
- Read this again, OIO is a valid cause for many ME/CFS cases and this has been reported in many studies. and there are many more. A microbiome shift is well documented in studies for ME/CFS and that by itself may be the cause of ongoing ME/CFS. Explicitly treating nutrient deficiencies is treating symptoms and not causes. Correcting the microbiome will likely resolve most, if not all, nutrient deficiencies. Microbiome dysfunction is well documented with anemia and thyroid dysfunction. A side effect taking the relevant antibiotic is microbiome correction. See Tess Falor’s experience above where remission came with concurrent normalization of the microbiome (corrected by the antibiotics — either directly or indirectly)
Q: Are you not aware of the black box warning of floxing [fluoroquinolone] with some of those antibiotics? Is this protocol target only for those who have lyme associated with the ME/ CFS. Cause most people in my medical community( not all have lyme)who took them have had horrible consequences from being floxed.
- Jadin was asked this question (see long video). She has never encountered this issue. It is critical to note HOW she uses it. Never more than 7 days followed by 3 weeks without antibiotics. For safety, she advises not to exercise while using it. Note that the warning also cites INJECTIONS as well as being seen after weeks on fluoroquinolone