
Recently I came across a PubMed article on iron deficiency with inflammatory bowel disease (IBD) which found “Shifts in gut bacterial diversity and composition associated with iron treatment are pronounced in IBD participants. Despite similar clinical outcome, oral administration differentially affects bacterial phylotypes and faecal metabolites compared with IV therapy…. Both per oral (PO) and IV treatments ameliorated iron deficiency, but higher ferritin levels were observed with IV…. PO treatment was associated with decreased abundances of operational taxonomic units assigned to the species Faecalibacterium prausnitzii, Ruminococcus bromii, Dorea sp. and Collinsella aerofaciens. ” [2016]
The superiority of IV over Oral with IBD is cited in other articles:
- “Intravenous iron treatment is better tolerated and more effective than oral iron treatment in improving ferritin.” [2012]
- “Patients who received IV iron had a greater rise in serum ferritin and were less likely to stop treatment due to adverse events, when compared with those who received PO iron.” [2015]
Iron and CFS
This appears to impact a subset of CFS patients.
- “The results indicate that [CFS] patients had significantly increased serum aluminum and decreased iron compared to controls. In the females, serum iron and dehydroepiandrosterone sulphate were significantly decreased and correlated.” [2001]
- “We reviewed, in this study, symptoms and syndromes associated with iron deficiency with or without anemia: fatigue, cognitive functions, restless legs syndrome, hair loss, and chronic heart failure. Iron is absorbed through the digestive tract. …Pathogenic micro-organisms or intestinal dysbiosis are suspected to influence iron absorption.” [2014]
- Iron insufficiency and hypovitaminosis D in adolescents with chronic fatigue and orthostatic intolerance [2011].
- “Although the cause of primary Restless legs syndrome (RLS) is still unknown, there is a strong connection between central metabolism of iron as well as dopamine levels and RLS manifestation.” [2011]
Probiotics and Iron
A quick summary is in “Gut microbes may play key role in iron status”
- Probiotic strain Lactobacillus plantarum 299v increases iron absorption from an iron-supplemented fruit drink: a double-isotope cross-over single-blind study in women of reproductive age[ 2015 ].
- The microbiota shifts the iron sensing of intestinal cells [2016]. “The amount of iron in the diet directly influences the composition of the microbiota. Inversely, the effects of the microbiota on iron homeostasis have been little studied….Commensal organisms (Bacteroides thetaiotaomicron VPI-5482 and Faecalibacterium prausnitzii A2-165) and a probiotic strain (Streptococcus thermophilus LMD-9) led to up to 12-fold induction of ferritin in colon.”
- “No significant differences were found between the two yogurts (one with live cultures and the other without) in terms of their effects on serum iron, AST and ALT levels.” [2013] – so only certain bacteria are involved.
- Probiotic bacteria reduce salmonella typhimurium intestinal colonization by competing for iron [2013]. “Thus, iron availability impacts S. Typhimurium growth, and E. coli Nissle reduces S. Typhimurium intestinal colonization by competing for this limiting nutrient.” – So E.Coli probiotics and iron deficiency may not play well together.
- ” Intestinal bacteria compete for the essential nutrient iron, leading to replacement of pathogenic Salmonella by the probiotic Escherichia coli Nissle, which is better equipped with iron acquisition systems, and resolution of infectious colitis.” [2013]
- Probiotics Lactobacillus reuteri DSM 17938 and Lactobacillus casei CRL 431 modestly increase growth, but not iron and zinc status, among Indonesian children aged 1-6 years [2013].
- Oral administration of Bifidobacterium longum CECT 7347 ameliorates gliadin-induced alterations in liver iron mobilisation [2013].
- “Bifidobacterium bifidum.. decreased amounts of calcium and iron released from bread.” [2012]
- “we show that a panel of probiotics are not able to respond to increased iron availability, and identify an isolate of Streptococcus thermophilus NCIMB 41856 that can increase growth rate in response to increased iron availability.” [2011]
- “Species of lactic acid bacteria that have been employed as probiotics were used. These were: L. bulgaricusJB005, L. casei JB006, L. casei JB008, B. animalis JB007, and B. bifidum JB009 (isolated from yoghurt); L. plantarum JB012 and L. helveticus JB012 (isolated from probiotic capsules); and the commensal isolates L. acidophilus ASF360 and L. salivarius ASF361 (components of the Schaedler flora). Two strains of S. thermophilus (JB004 and NCIMB 41856) were isolated from yoghurt. Two strains of AIEC were used: HM427 and HM615 (kindly provided by Dr Barry Campbell and Prof Jon Rhodes, University of Liverpool), as was E. coli K12 and E. coli Nissle 1917 (isolated from Mutaflor (Ardeypharm GmbH, Herdecke, Germany)).”
Bacteria and Iron
I have heard people express the opinion that some bacteria, like Lyme, need iron, that you should avoid iron supplements. To me this is a gross and perhaps, dangerous simplification. It is like saying, “Mafia are Italians, so to solve the Mafia problem, we need to deport all of the Italians” (or Japanese, or Muslims, or…).
“A Syracuse University research team… discovered that some bacteria are equipped with a gene that enables them to harvest iron from their environment or human host in a unique and energy efficient manner.”[2008] Thus an overgrowth of Actinomycetes may result in iron deficiency.
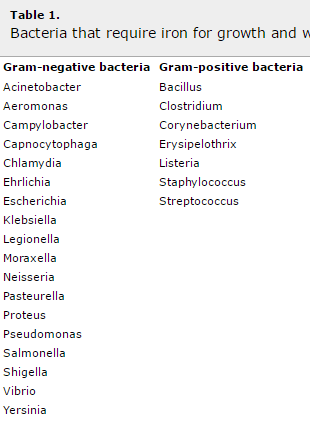
Below is a table from [2006], some strains are good and other are bad. “Macrophages use iron for production of hydroxy-radical and superoxide reactions, which are necessary for microbial killing. Presumably, as a survival strategy, bacteria, which also require iron for survival, have adapted the ability to sequester iron from the host, thereby limiting the availability to macrophages.” [2007]
Bottom Line
First thing is that you cannot deal with all issues at the same time. You must choose which one you will direct your efforts towards improving. The gut bacteria dysfunction was a cascade of changes, and unwinding it means addressing one issue at a time. Where to start? There is no literature indicating the fulcrum that should be our start point — so my suggestion is simple: the very worst symtpom!!
If you have low iron and thus tiredness, low hemoglobin (and thus oxygen), insomnia, etc, you may wish to try to address that first. From the literature above, besides eating iron rich food, you should take, if available:
- Streptococcus thermophilus NCIMB 41856 [Patent] – may be available soon
- Lactobacillus plantarum 299v – Jarrow brand, available on Amazon, and in Sweden as “ProViva Naturell Filmjölk”
- Bacteroides thetaiotaomicron VPI-5482
- Faecalibacterium prausnitzii A2-165
- Streptococcus thermophilus LMD-9
Streptococcus thermophilus is in most yogurts (see Probiotic Yogurt for a list, for example Chobani contains none), the problem is usually which strain is used!
You should also consider taking IV Iron, it improves the gut bacteria more than oral iron. In general, “The present results suggest that Fe[Iron] supplementation enhances the concentration of beneficial gut microbiota metabolites and thus may contribute to gut health.” [2014]
Note that all of these are specific strains. Streptococcus thermophilus JB004 did not show strong effects.
You should also avoid Mutaflor, Symbioflor-2, Bifidobacterium bifidum which will decrease iron availability.
