A reader forwarded me two reports, one from a male and one from a female. No notes on the people (I am fine with that). The report appear to be superior to uBiome on two counts:
- It’s a professional grade report from a clinical laboratory
- It reports down to the strain level on occasion.
Link to site (in Italian) http://www.ospedalebambinogesu.it/genetica-la-super-mappa-del-microbiota-intestinale#.Wf39d2i3xPY
This first post is on the female. (See this post for the male)
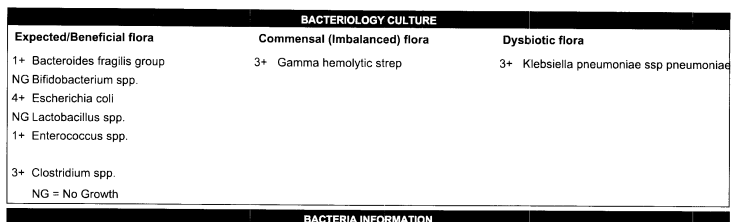
- Low Bifidobacteria
- No Lactobacillus
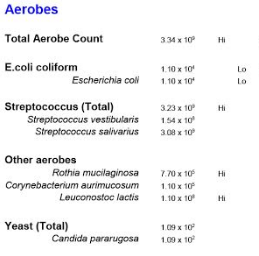
- No E. coli
- Low Akkermansia muciniphila (less than 1/100 of 1% of typical)
So standard CFS profile on these

Copying the data to Excel allow me to get similar numbers as I do from uBiome reports.
High Levels
| Proteobacteria | Haemophilus parainfluenzae | 75956% | 0.06836 |
| Firmicutes | Ruminococcus torques | 11110% | 0.00222 |
| Firmicutes | Veillonella dispar | 1819% | 0.01473 |
| Firmicutes | Ruminococcus gnavus | 1720% | 0.03956 |
| Firmicutes | Epulopiscium dolichum | 891% | 0.00196 |
| Firmicutes | Coprobacillus | 880% | 0.00044 |
| Firmicutes | Blautia producta | 853% | 0.00665 |
| Firmicutes | Clostridium | 721% | 0.00281 |
| Firmicutes | Ruminococcus | 268% | 0.09076 |
| Firmicutes | Epulopiscium | 220% | 0.00011 |
The greatest impact appears to be (in order) from Ruminococcus, Haemophilus parainfluenzae, Ruminococcus gnavus, Veillonella dispar. Since I have only done deep dives to the genus, not species level, I have borrowed directly from DataPunk.Net
- Ruminococcus: https://cfsremission.wordpress.com/2017/10/18/reducing-ruminococcus-genus/
-
Proteobacteria -> Gammaproteobacteria -> Pasteurellales -> Pasteurellaceae -> Haemophilus -> Haemophilus parainfluenzae
- Firmicutes -> Clostridia -> Clostridiales -> Lachnospiraceae -> Blautia -> Ruminococcus gnavus
- Firmicutes -> Negativicutes -> Selenomonadales -> Veillonellaceae -> Veillonella -> Veillonella dispar
- INHIBITED BY
- ENHANCED BY
- Firmicutes -> Clostridia -> Clostridiales -> unclassified Clostridiales -> Epulopiscium -> Epulopiscium dolichum
- NOTHING
- Firmicutes -> Erysipelotrichia -> Erysipelotrichales -> Erysipelotrichaceae -> Coprobacillus (Pending deep dive)
- Firmicutes -> Clostridia -> Clostridiales -> Lachnospiraceae -> Blautia -> Blautia producta
- Clostridium : https://cfsremission.wordpress.com/2017/10/07/decreasing-clostridium-genus/
- Firmicutes -> Clostridia -> Clostridiales -> unclassified Clostridiales -> Epulopiscium
- Nothing
Bottom Line
Combining all of the lists and tossing out things that appear on both side, we have the following lists. There are two genus cited above that I have not done a deep dive into. I have skipped rare bacteria because of the number of over growths found. This was a pretty clean merge — often the same item appeared multiple times in one list or the other.
The lists below are done by merging the lists from the deep dives linked above. Some items may encourage one genus and discourage another genus — those are placed in inconclusive. The impact on Lactobacillus, Bifidobacterium and E.Coli are intentionally ignored [See this post for the logic]. This is all based on applying logic to the results of studies — thus theoretical. This is an addition (not a replacement) to this overview post.
Avoid
- Proton-pump inhibitors (PPI) Cholic acid
- Berberine
- Resistant starch (type II, IV)
- Gynostemma pentaphyllum (Southern Ginseng or Jiaogulan) — not related to regular ginseng)
- Partial Sleep Deprivation
- Polysorbate 80
- Soy
- Polydextrose
- Resistant maltodextrin.
- Lactobacillus acidophilus
- Lactobacillus rhamnosus GG
- β-Glucan / Barley
- Saccharomyces boulardii
- Bifidobacterium animalis
Take
- Cranberry bean flour
- Flaxseed
- Navy bean (Cooked)
- Thyme oil
- Perilla oil
- Peppermint oil
- Lemongrass oil
- Coriander oil
- Lavender (spike) oil
- Lactobacillus salivarius
- Lactobacillus paracasei
- High fat/meat diet
- Gallate (Green Tea)
- Bifidobacterium longum and Bifidobacterium Breve
- Bacillus licheniformis (it does produce histamines, see this post)
- Lactobacillus casei probiotics
- Lactobacillus kefiri LKF01
- Lactobacillus rhamnosus probiotics
- Prescript Assist Probiotics
- Streptococcus Probiotics
- Chitosan supplements
- Have Chocolate!
Note: Taking as a fresh herb may work similar to oil
This is an education post to facilitate discussing this approach with your medical professionals. It is not medical advice for the treatment of CFS. Always consult with your medical professional before doing any changes of diet, supplements or activity. Some items cites may interfere with prescription medicines.