This is a continuation of my last post looking at other conditions where there is evidence of DNA + Microbiome shift causing a disease. With CFS, the shift has started and may progress into other diseases.
Rheumatoid Arthritis
Microbiome
- “colonization of particular intestinal bacteria was sufficient to induce arthritis.” [2016]
- “A growing number of microbiota constituents such as Prevotella copri, Porphyromonas gingivalis, and Collinsella have been correlated or causally related to rheumatic disease.” [2016]
- “The results of biological research of colon microbiota of patients with rheumatoid arthritis (RA) is in article presented. The signs of III degree dysbiosis, by reducing the concentration of Bacteroides spp., Bifidobacterium spp., Lactobacillus spp. populations, typical strain E. coli. But over growth of populations Klebsiella spp., Proteus spp., Staphylococcus spp., atypical forms of E. coli, Candida spp. The scheme for the correction of the colon microflora of patients with (RA) by was proposed bifiform. Increasing of populations concentration of Bifidobacterium spp., Bacteroides spp., Lactobacillus spp., typical E. coli, Enterococcus spp. and selective decontamination of Enterococcus (Hly+), Klebsiella spp., Proteus spp., Staphylococcus spp., lactosonegative and E.coli (Hly+) confirmed after using of this eubiotics.” [2014]
- Treatment of adjuvant-induced arthritis with the combination of methotrexate and probiotic bacteria Escherichia coli O83 (Colinfant) [2009].
- “Our results indicate that Enterococcus faecium may increase the preventive effect of methotrexate treatment in rat adjuvant arthritis by improving its anti-inflammatory and antiarthritic effects.” [2005]
- ” A growing body of evidence has shed light on the association of dysbiosis of gut microbiota with RA. Certain gut microbial strains have been shown to inhibit or attenuate immune responses in RA experimental models, suggesting that specific species among intestinal commensal bacteria may play either a pathogenic or a protective role in the development of RA.” [2016]
- “Patients with RA exhibited decreased gut microbial diversity compared with controls, which correlated with disease duration and autoantibody levels.A taxon-level analysis suggested an expansion of rare taxa, Actinobacteria,…The abundance of Collinsella correlated strongly with high levels of alpha-aminoadipic acid and asparagine as well as production of the proinflammatory cytokine IL-17A. A role for Collinsella in altering gut permeability and disease severity was confirmed in experimental arthritis.” [2016]
- “A subpopulation of patients with early RA harbored intestinal microbiota dominated by Prevotella copri;” [2016]
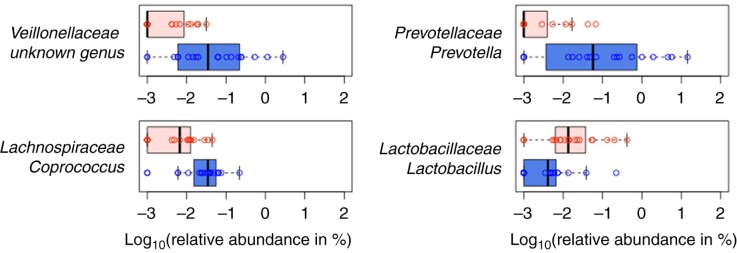
- “Mice susceptible to collagen-induced arthritis (CIA) showed enriched operational taxonomic units (OTUs) affiliated with the genus Lactobacillus as the dominant genus prior to arthritis onset. With disease development, the abundance of OTUs affiliated with the families Bacteroidaceae, Lachnospiraceae, and S24-7 increased significantly in CIA-susceptible mice….Due to the extreme complexity and diversity of the gut microbiome, it is unlikely that differences in the abundance of a single species are responsible for differences in RA susceptibility. Rather, these differences most likely result from context-dependent interactions among the multiple species constituting the gut microbiota.” [2016]
- “The results of this study indicate that the oral intake of probiotic B. coagulans and prebiotic inulin can improve the biochemical and clinical parameters of induced RA in rat.” [2016] [2010]
- “Conclusion: Lactobacillus casei 01 could not improve serum lipids in RA patients.” [2017]
- “probiotics — Lactobacillus rhamnosus GR-1 and Lactobacillus reuteri RC-14 capsules administered orally. — did not clinically improve RA as measured by the ACR20,”
- “Subjects who received probiotic capsules – Lactobacillus acidophilus (2 × 10(9) colony-forming units [CFU]/g), Lactobacillus casei (2 × 10(9) CFU/g) and Bifidobacterium bifidum (2 × 10(9) CFU/g) for 8 weeks. — experienced borderline statistically significant improvement in total- (P = 0.09)” [2016]
- “there were no statistical significant differences in the activity of RA, more subjects in the Lactobacillus rhamnosus GG (LGG) group reported subjective well being.” [2003]
DNA / SNP
- Polymorphisms of RAD51B are associated with rheumatoid arthritis and erosion in rheumatoid arthritis patients [2017].
- Associations between C677T and A1298C polymorphisms of MTHFR and susceptibility to rheumatoid arthritis: a systematic review and meta-analysis [2017].
- Polymorphism and protein expression of MUTYH gene for risk of rheumatoid arthritis [2017].
- Significance of Polymorphism and Expression of miR-146a and NFkB1 Genetic Variants in Patients with Rheumatoid Arthritis [2016].
Bottom Line
The over abundance of Lactobacillus immediately before onset, and no really significant results from any Lactobacillus probiotics strongly suggests that all Lactobacillus probiotics should be avoided.
E.Coli probiotics [Colinfant, Symbioflor-2, Mutaflor] and Bacillus probiotics are what studies suggest are most likely to help. Second line would be: Bifidobacterium spp., Bacteroides spp., Enterococcus spp.