In my last post, we found that probiotics may last for just hours or months – depending on the sourcing and type of bacteria. Probiotic behaviors vary greatly. Some produce natural antibiotics that will kill off other species. Others do not — just reduce inflammation etc. or grow more aggressively than bad bacteria. Some commercial probiotics are documented in FDA filing to be easily killed by almost all antibiotics, not to persist and not to produce toxins against other bacteria (good or bad).
We have limited knowledge of which ones produces natural antibiotics, so my rule of thumb is that probiotics should be viewed as producing antibiotics. You should rotate them regularly to prevent resistance to their natural antibiotics occurring. The same applies to herbs. Changing providers when you finish a herb is similarly desired.
The lack of (successful) studies on fixing dysfunctional microbiome
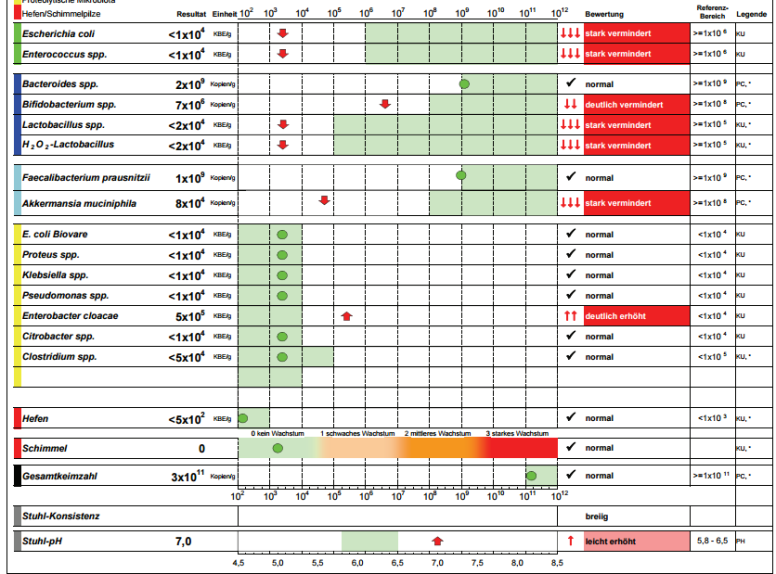
My model appears to be well supported by Kyberkompact lab results, published papers over seventeen (17) years, etc.
- ” In contrast, in the stool samples there was a higher relative abundance of Bacteroidetes and lower abundance of Firmicutes observed in ME/CFS patients compared to healthy controls.” [2015]
- ” For the anaerobes, the mean percentage distribution of Bacteroides spp. for the control subjects and CFS patients was 92.8% and 91% respectively; Bifidobacterium spp, 7.1% and 2%; Lactobacillus spp., < 1% and 0%. The incidence of CFS patients with faecal E.coli greater than the percentage mean of control subjects was significantly different to that of the Bacteroides spp. (7 vs 21 respectively, p=0.0001) suggesting the possibility of an antimicrobial interaction among bacterial species.” [1998]
What is lacking are studies showing consistent successful treatment that persists.
- “The high success rate and safety in the short term reported for recurrent Clostridium difficile infection has elevated Fecal microbiota transplantation (FMT) as an emerging treatment for a wide range of disorders, including Parkinson’s disease, fibromyalgia, chronic fatigue syndrome, myoclonus dystopia, multiple sclerosis, obesity, insulin resistance, metabolic syndrome, and autism.” [2016]
- I have corresponded with several people that had them, went into remission for months and then relapses
- “Case reports of FMT have also shown favorable outcomes in Parkinson’s disease, multiple sclerosis, myoclonus dystonia, chronic fatigue syndrome, and idiopathic thrombocytopenic purpura. FMT is a promising approach in the manipulation of the intestinal microbiota and has potential applications in a variety of extra-intestinal conditions associated with intestinal dysbiosis.” [2015]
- “This raises the question of whether restoration of a healthy microbiome via probiotics or other ‘dysbiosis therapies’ would be an optimal alternative, or parallel treatment option, to antibiotics.” [2016]
- “The use of specific probiotics in patients with IBD can be recommended only in special clinical situations. There is no evidence for efficacy of probiotics in CD. By contrast, studies in UC have shown a beneficial effect in selected patients.” [2016]
My approach
The use of antibiotics must be divided into two groups:
- Acute infection treatment – typically resolved by a single course of antibiotics over 2 weeks with a focus on a single bacteria.
- Latent/chronic/persistent/occult infections – which are complex to treat.
It is the latter that is needed for CFS, FM and many autoimmune diseases. We are not trying to eliminate one bacteria but reduce dozens of families while increasing dozens of families. When some of the counts for families are reduced to 1% of normal or even 1% of 1% (1/10000), getting those counts up is a challenge, a 400% increase of some counts do not even touch the dysfunction.
We do not know the complete complex interactions between strains, species and families of bacteria. We try to change one item and the side-effects may leave the patient worst.
How to proceed?
My approach comes from being placed successfully into remission three times using rotating antibiotics. The first time, before CFS was a clinical diagnosis (in 1972-3, Incline Village was in 1984) and the physician went with the diagnosis of antibiotic resistant walking pneumonia – rotating antibiotics when one course did not resolve it. The latter two times, modelling treatment on Dr. Cecile Jadin’s protocol for occult rickettesia infections (although my medical records for the last time read chronic lyme).
Bacteria mutate and become resistant. You may eliminate 99%, but if the environment supports growth, that 1% grows quickly and the volume returns. Our goal is to reduce parts of this consortium of evil bacteria until the good bacteria can muscle back in. Each herb, probiotic or antibiotic will only influence a few families of bacteria. You can knock those back and then reduce their friends, and then their friend’s friends.
There is a little literature on rotation:
- “This review provides an overview of… antibiotic rotation as strategies to modulate antibiotic resistance in the intensive care unit.” [2015]
- “Furthermore, improvements in clinical practice, rotation of antibiotics, herbal drugs, nanoantibiotics and the development of newer antibiotics based on a pharmacogenomic approach may prove helpful to overcome dreadful vancomycin-resistant enterococcal infections.” [2014]
- Antibiotic rotation strategies to reduce antimicrobial resistance in Gram-negative bacteria in European intensive care units: study protocol for a cluster-randomized crossover controlled trial [2014]
- Implementation of antibiotic rotation protocol improves antibiotic susceptibility profile in a surgical intensive care unit. [2007]
- “A 65.9% reduction in the use of cefepime occurred after the antibiotic rotation. In the surveillance stool cultures, the detection rate of cefepime-resistant gram-negative isolates, of which ESBL-producers were predominant, declined significantly after the intervention (8.5 vs 0.9 episodes per 1000 patient days before and after intervention respectively, P<0.01).” [2013] – A 90% drop in episodes
- Rotating antibiotics selects optimally against antibiotic resistance, in theory[2010.
Pulsing
Pulsing is much less studied. If you rotate, you are in one sense pulsing. Again, very little literature because for most infections – a single course of antibiotics is sufficient to knock out one bacteria.
“The issue of whether it is better to administer antibiotics as an intermittent bolus dose or a continuous intravenous infusion has been debated for several decades.” [1988]
- My own experience has been modeled on Jadin’s protocols (See this summary)
- “While this study does not demonstrate a superior response to dosing metronidazole in a pulsatile fashion against B. fragilis and B. thetaiotaomicron isolates, the effect is comparable to that of conventional dosing regimens. Perhaps this novel dosing strategy would prove advantageous against other pathogens.” [2004] – no worst than taking it constantly etc.
- “In the current study, use of pulsatile dosing against S. pneumoniae with reduced susceptibility demonstrates superior reduction in bacterial concentration compared to that of more traditional two- or three-times-daily dosing. However, further research exploring the mechanism for pulsatile dosing and confirmation of these results are needed before applying this information clinically.” [2006]
- “Overall bacterial density reduction was similar between the regimens for the susceptible isolate and greater with pulsatile regimens against the less susceptible strain.” [2004] – pulsing works better when the bacteria is more resistant.
- A 2012 mathematical modeling study pulsing may be the preferred application of anti-pathogens: “We find that constant dosing is not the optimal method for disinfection. Rather, cycling between application and withdrawal of the antibiotic yields the fastest killing of the bacteria.”
Bottom Line
I advocate rotation and/or pulsing. See earlier post from 2015. The key for knowledgable medical professional to grasp is that we are not dealing with a infection of a single bacteria (classic) but overgrowths of dozens, perhaps hundreds of bacteria families. We need to correct the shift… and that is far more complex.
How long should I take one thing? IMHO: 2 weeks minimum (typical course of antibiotics duration), 4 weeks maximum.