
I thought it would be good to review some of the hundreds of studies published on PubMed in 2016 to see if anything especially interesting has been published.
- “During life, the numbers of bifidobacteria decrease from up to 90% of the total colon microbiota in vaginally delivered breast-fed infants to <5% in the colon of adults and they decrease even more in that of elderly as well as in patients with certain disorders such as antibiotic-associated diarrhea, inflammatory bowel disease, irritable bowel syndrome, obesity, allergies, and regressive autism.” [2016]
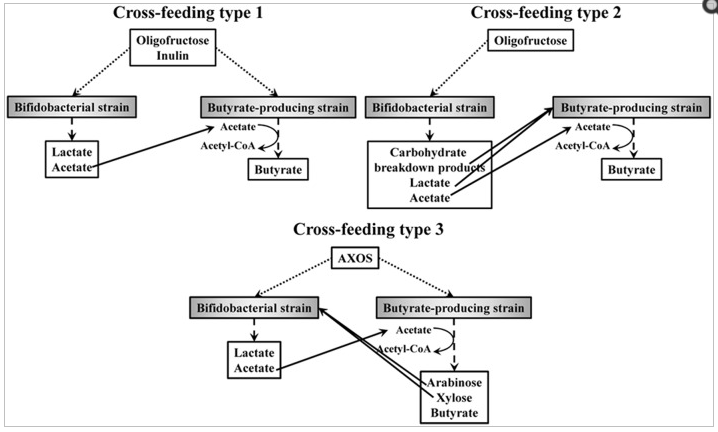
- ” Butyrate is an essential metabolite in the human colon, as it is the preferred energy source for the colon epithelial cells, contributes to the maintenance of the gut barrier functions, and has immunomodulatory and anti-inflammatory properties. It has been shown that the butyrogenic effects of ITF and AXOS are the result of cross-feeding interactions between bifidobacteria and butyrate-producing colon bacteria, such as Faecalibacterium prausnitzii (clostridial cluster IV) and Anaerostipes, Eubacterium, and Roseburia species (clostridial cluster XIVa). These kinds of interactions possibly favor the co-existence of bifidobacterial strains with other bifidobacteria and with butyrate-producing colon bacteria in the human colon.” – hence Clostridium butyricum (Miyarisan) probiotics may be a very significant factor.
- AXOS => arabinoxylan-oligosaccharides
- “Low-FODMAP rye bread helps IBS patients to control their symptoms and reduces gastrointestinal gas accumulation.” [2016] I have been a long time advocate of 100% rye bread (with zero wheat flour in it) – 100% rye bread encourage biodiversity, [2012].
- “a newly emerging condition termed non-celiac gluten (or wheat) sensitivity[NCGS/NCWS] is now well established in the clinical practice. Notably, patients with NCGS/NCWS have symptoms that mimic those present in irritable bowel syndrome.” [2016] – IBS does not mean wheat (or gluten) sensitivity. Many “gluten sensitive” individuals are actually wheat sensitive only.
- “Using strict criteria as recommended for IBS studies, about one third of patients with IBS-D or IBS-M are wheat sensitive, with a similar proportion in both IBS types. ” [2016]
- “Of 1074 patients (44.1%) who responded to open-label rifaximin, 382 (35.6%) did not relapse, whereas 692 (64.4%) did; of these, 636 were randomly assigned to receive repeat treatment with rifaximin (n=328) or placebo (n=308). The percentage of responders was significantly greater with rifaximin than placebo (38.1% vs 31.5%, P=.03). The percentage of responders for abdominal pain (50.6% vs 42.2%, P=.018) was significantly greater with rifaximin than placebo, but not stool consistency (51.8% vs 50.0%, P=.42).” [2016] So Rifaximin helps about 1/3 of IBS patients – but this amounts to actually just 7% (38% improved with Rifaximin, and 31% improved with a placebo — 38% – 31% = 7%) … so real odds is closer to 1/14.
- “More than every tenth Dane have irritable bowel syndrome. The condition is diagnosed by a positive strategy including fulfilment of the Rome III criteria, absence of alarm symptoms, and if needed a few paraclinical tests. Currently, there is no cure of the disorder. Treatment is recommended on a symptom-based approach targeting the dominating symptom/symptoms. If symptoms are reduced, the quality of life is considerably improved.” [2016]
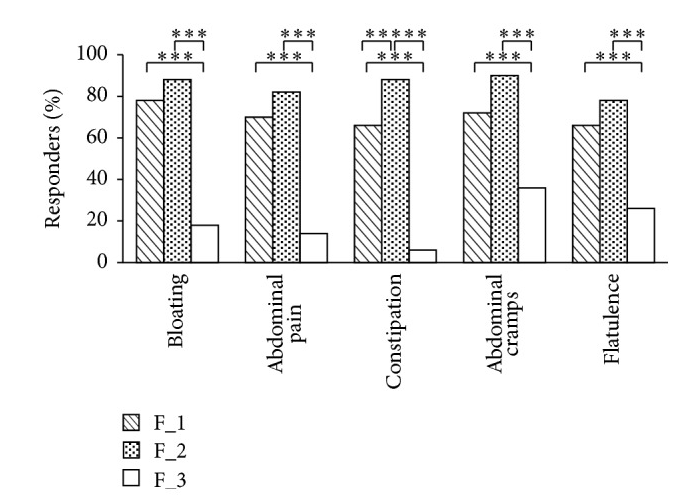
- “Multispecies probiotic supplementations are effective in IBS-C subjects and induce a different assessment in the composition of intestinal microbiota” [2016]
- “it is known that the level of bifidobacteria and lactobacilli species is lower in IBS patients compared to healthy persons [28, 29] and several studies show that the supplementation of them, or mixtures including species of these genera, is effective in alleviating symptoms of IBS. Moreover, the selected strains were already known for their effect on intestinal cell lines as previously reported [19].”
- Mixture F_1: 5 × 109 CFU L. acidophilus , 5 × 109 CFU L. reuteri (30 mg as lyophilized), – 10 Billion CFU
- Mixture F_2: 5 × 109 CFU L. plantarum, 5 × 109 CFU L. rhamnosus , 5 × 109 CFU B. animalis subsp. lactis – 15 Billion CFU BEST – see posts on L.Rhamnosus
- Mixture F_3: 390 mg inulin (almost a Placebo)
- “self-reported anxiety and depression provide a twofold risk for IBS onset.” [2016]
- “Species richness, but not community diversity, differentiated all IBS patients from Healthy Controls.” [2016]



