A reader wrote to me
Hi Ken,
So I had my first sinus / ear infection in years and was put on Augmentin. Within 24 hours, I was feeling better than I have in years. That has continued somewhat the whole course of treatment, though I only have a few days left.
I think it’s possible to use your site to see what a specific antibiotic might be doing to the microbiome? Can you do a walkthrough? Maybe I can replicate the effect Augmentin is having with supplements, probiotics and food since my last microbiome test is over a year old now.
Always striving…
This type of email, describing feeling better on some antibiotics, I have seen many, many times from people with ME/CFS. The problem is physicians will prescribe antibiotics for other issues, for example Acne, but not for severely life-changing conditions like ME/CFS.
I have one more question, for example if I want to replace the fluoroquinolones antibiotic class with a herb or herbs, can I use your website to find a “replacement” that would have a similar impact on the microbiome ? If yes, how would I do that ?
From a different reader in this morning’s emails. With a specific microbiome, it can be inferred – but in terms of a generic equivalent … antibiotics impact too many things to get a reasonable replacement of herbs and spices.
This reader asked something which was an elegant request, “replicate the effects of the antibiotics”. After some experiments, I discovered that it was possible and just finished creating a page.
- A microbiome (16s) is needed before the antibiotics
- The name of the antibiotic
Verbal Description of the Steps
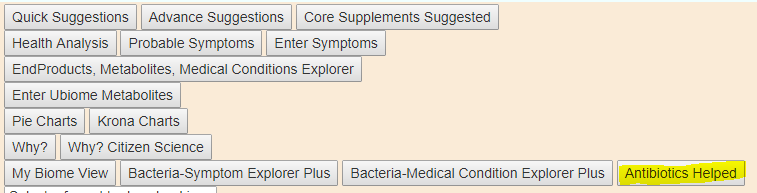
- Log on to the site, you will see a new button [Antibiotics Helped]
A new page appears, type in the name of the antibiotic, perhaps with ‘%’ around it to do a general search

You may get multiple items, usually brand names for the same thing,

Check the item desired (only one is allowed), THEN pick the microbiome sample you used. Click the button if needed.

A new page will appear. This consists of the bacteria impacted by this antibiotic and what you had. The person may have 500 taxa, the antibiotic may have 60 taxa, what is in common (the “intersection”) may be just 30 taxa. The items that are in common are what is shown.

Inspect the candidates, and put a check box by the ones you wish to include. Then click add to hand picked taxa. This will send you back to the samples page. On this page you will see a golden line of buttons appear.

Click View to see what was added:

Return, and then try the golden suggestions buttons. I first did it with just herbs and antibiotics to see if there are alternative antibiotics, and more important, where did my antibiotic show up in the rankings

That’s it. A video with more discussion is below.
ADDENDUM 1
A reader pointed out that this can be used for screening / testing for likely side-effects on the microbiome BEFORE taking! An example is shown below


ADDENDUM 2
I decided to make available under the DEMO login, my microbiome from early in my ME/CFS relapse. The microbiome may not apply to you — but if you are looking for herbs, spices etc for fluoroquinolones and minocycline, Zithromax, etc and DO NOT have a microbiome sample, then it is likely better than no information. From my experience with various antibiotics, some work very well and others “so-so”
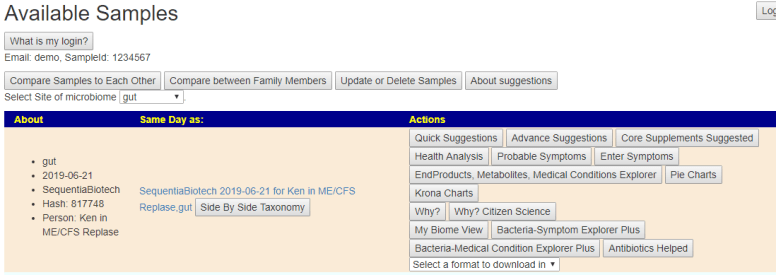
If anyone else wishes to share one of their samples for a specific condition, feel free to email me. I will change the email to “demo” and update the person information in the database to preserve your privacy.