
I have just created a new set of pages to allow people who have done uBiome to share the metabolism information that is also provided there. I put my own and a friend’s thru and was struck by the differences. Almost all of mine was sitting at .95 – 1.05 of normal. Many of her’s were sitting at 0.03, 0.05 of normal.
Short Explanation
Bacteria have a large number of interactions and behaviors. There is a site where this information has been gathered, KEGG PATHWAY Database. uBiome has used this site with your bacteria sample to predict/estimate how well various pathways are working with your current bacteria mixture.
You will find this information under [Advance] on your uBiome page
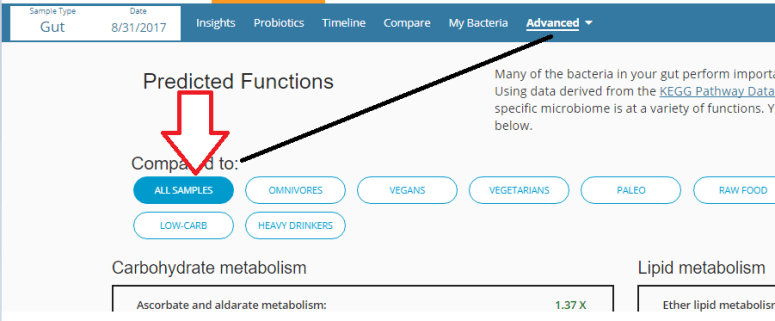
There is no ability to download and upload it at present. The items are arrange from highest to lowest value.
I have created an entry page (AFTER YOU LOGIN and pick the sample) at: http://ubiomecfsweb.azurewebsites.net/Metabolite/metabolismEntry
The page is shown below. I have chunked ranges together to make entry easier.
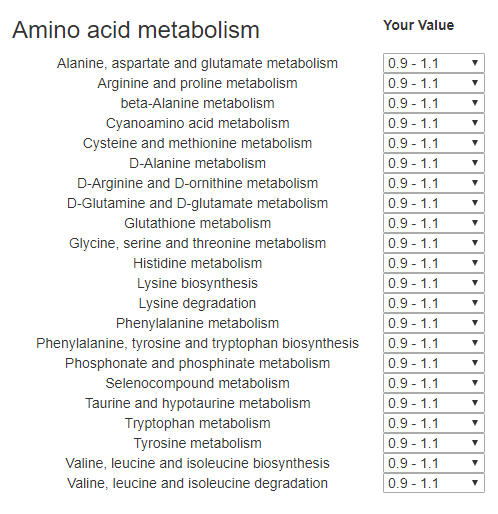
In general, we are concerned about low values. What the values means and what you can do about them will be covered in later posts when we get data.
Examples:
- A low “Ubiquinone and other terpenoid-quinone biosynthesis” means that your bacteria under produces Ubiquinone (a.k.a. CoQ10) and thus you should be supplementing with it — perhaps in higher dosages than usual.
- A low “Styrene degradation” means that you may need to really avoid items with even trace amount styrene, in fact, “The U.S. Environmental Protection Agency (EPA) has described styrene to be “a suspected toxin to the gastrointestinal tract, kidney, and respiratory system, among others”.[29][30] ” which may be a contributing factor for IBS
- A low “Retinol metabolism” (Vitamin A), means it takes longer for the body to use it. In some cases if it is water borne, then you may urinate it out unprocessed and have little effect from a normal dosage.
I will likely do deep dives into these — every 5 sets submitted will result in the lowest common values seen being the next deep dive.
A video
For more videos, go to this page.
Bottom Line
Adding metabolites WITH symptoms may help discover association between chemical sensitivity and the metabolic functioning, etc. We need uBiomes, symptoms and metabolites to obtain a rich set of data to identify symptoms to both bacteria and to metabolites (i.e. hints to the specific supplements that may help you!)
I have also stubbed out a symptoms to metabolite explorer page.
GENDER AND AGE Has Been Added to Symptoms
If you have entered symptoms, please update it with your gender and age.
 Bottom Line
Bottom Line