My answer is simple: Yes — but the mechanism may be one of several possible. The most likely are:
- Environmental influences.
- Family behavior patterns (i.e. stress level run high)
- Explicit DNA Mutations
- Shared microbiome signatures
Despite a prevalence of ∼0.2-0.4% and its high public health burden, and evidence that it has a heritable component, ME/CFS has not yet benefited from the advances in technology and analytical tools that have improved our understanding of many other complex diseases.
Genetic risk factors of ME/CFS: a critical review [2020]
Some paediatricians will have noted a family history of CFS/ME and may have wondered whether this was due to genetic heritability or an environmental factor.
Is chronic fatigue syndrome (CFS/ME) heritable in children, and if so, why does it matter? [2007]
A heritable component is implicated by the reported increased risk in relatives of ME/CFS patients [10,11,12], and genetic association studies are emerging in order to identify risk variants. We have recently reported associations with specific HLA alleles, HLA-C*07:04 and HLA-DQB1*03:03 [13], and individuals carrying either one or both risk alleles seem to more often respond positively to the immunosuppressive drug cyclophosphamide [14]
No replication of previously reported association with genetic variants in the T cell receptor alpha (TRA) locus for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) [2022]
Let us take these in reverse order.
Environmental influences
A simple example is a house with a mold issue. The parents may be impacted by the mold, and it is likely that the children will also be impacted. Recently I saw that mites (Chiggers) can spread disease causing bacteria. If one in the household has an asymptomatic infection, it may well spread to others in the family. The household may live in an area where there is pesticide drift. The sensitivity to these factors may be genetic or epigenetic. An environment factor that pre-dispose one child to ME/CFS will likely influence other children of the same family.
“Research to date has demonstrated the initiation of neurobehavioral sensitization by volatile organic compounds and pesticides in animals, as well as sensitizability of cardiovascular parameters, beta-endorphin levels, resting EEG alpha-wave activity, and divided-attention task performance in persons “
Family behavior patterns (i.e. stress level run high)
Domestic abuse can be both spousal and parental (and even siblings). Abuse (and stress) increases the risk of ME/CFS. A person that is abused is more likely to become an abuser (hence passing through generations) See Intergenerational Trauma: How Child Abuse Patterns Repeat Across Generations [2018]
- The association between exposure to domestic abuse in women and the development of syndromes indicating central nervous system sensitization: A retrospective cohort study using UK primary care records [2021]
- Intimate Partner Violence and the Risk of Developing Fibromyalgia and Chronic Fatigue Syndrome [2021]
- Psychiatric disorders and the onset of self-reported fibromyalgia and chronic fatigue syndrome: The lifelines cohort study. [2023]
An additional dimension is personality types, which also runs in families
- [Relationship between chronic fatigue syndrome and type A behaviour] [2009] – ME/CFS are more Type A.
Explicit DNA Mutations
This actually has at least two subsets. Defects causing hypercoagulation and general ME/CFS ME/CFS population is the one that I am more, if too familiar with. The general population is prone to a large amount of noise and typical finding is that a third or less of ME/CFS patients have a relevant mutation, while the same mutation is seen only half as often in the general population. This means that 2/3 of ME/CFS patients will not have this mutation – so limited value for making a diagnosis. If you have a specific mutation that is known to be treatable, then that should be factored in.
- Genetic association study in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) identifies several potential risk loci [2022] Weak evidence:
- rs2582085, rs115523291, rs8108136, rs6089982
- No replication of previously reported association with genetic variants in the T cell receptor alpha (TRA) locus for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) [2022]
- Fine mapping of the major histocompatibility complex (MHC) in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) suggests involvement of both HLA class I and class II loci [2021]
- rs4711249, rs9275582
- Human Leukocyte Antigen alleles associated with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) [2020] Weak evidence
- “The proportion of individuals carrying one or both of these alleles was 19.2% in the patient group and 12.2% in the control group “
- Association of chronic fatigue syndrome with human leucocyte antigen class II alleles [2005]
- Weak: Found in 30.2% of patients v 20.0% of control;
- [Identification and application of marker genes for differential diagnosis of chronic fatigue syndrome] [2007] “Reported genes were mostly different from the previously reported genes, again featuring the complexity of CFS. Separately, we identified 9 genes that were significantly and differentially expressed between CFS patients and healthy subjects using an original microarray”
When more complex statistical methods are used, Prediction of complex human diseases from pathway-focused candidate markers by joint estimation of marker effects: case of chronic fatigue syndrome [2015] this “resulted in 80% accuracy, one of the best so far for CFS in comparison to previous prediction models.” This approach does not look for a single mutation but for combinations of many different mutations. Each one of these contributes a little.
The hypercoagulation SNP is different because you are not looking for a mutation shared by all ME/CFS patients but mutations already known to encourage coagulation. Dave Berg pioneered this work.
- The Occurrence of Hyperactivated Platelets and Fibrinaloid Microclots in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) [2022]
A partial list of these SNPs are in my 2015 post, Snps for Coagulation Defects. To these, we can add the following:
- Missense Variants of von Willebrand Factor in the Background of COVID-19 Associated Coagulopathy [2023]
- vWF (rs216311, rs216321, rs1063856, rs1800378, rs1800383). “Our results imply that missense vWF variants might modulate the thrombotic risk in COVID-19.”
- Contribution of the von Willebrand factor/ADAMTS13 imbalance to COVID-19 coagulopathy [2022]
Shared microbiome signatures
Bacteria may be transferred by a kiss or even touching. Similar diets will encourage the same profiles. Like the environment, it may pre-dispose people in the same family because of the shared food, and the shared microbiome.
- Gut microbiota metabolites mediate the interplay between childhood maltreatment and psychopathology in patients with eating disorders [2023] – so abuse in a family also alters the family’s microbiomes.
- Metagenomic analysis of mother-infant gut microbiome reveals global distinct and shared microbial signatures [2021]
- Studying Vertical Microbiome Transmission from Mothers to Infants by Strain-Level Metagenomic Profiling [2017]
With this less documented dimension, the microbiome may be pre-disposed towards being dysfunctional. Similarly, the microbiome may pre-dispose a person to have high anxiety. Things become a bit more complicated because the microbiome is influence by DNA (and the reverse). There was a Chinese study that I remember reading where both COVID severity and Long COVID was associated with people’s pre-COVID microbiome (they happen to have been running a large time-lapse study on the microbiome)
Bottom Line: It does run in Families
My suggestion for action plans for those concerned:
- Improve the environment as much as is possible.
- Reduce the exposure to pesticides and man-made chemicals (for example fragrances). It is very common for ME/CFS people to develop acute sensitivity to many chemicals which hints that they may be a contributor to the condition.
- Check for molds and fungi. Monitor the humidity levels in your living space and take action as needed
- Urban air pollution has also been implicated.
- Associations between Unconventional Natural Gas Development and Nasal and Sinus, Migraine Headache, and Fatigue Symptoms in Pennsylvania. [2017]
- If type-A personality or high anxiety is a factor, learning better coping mechanisms or lowering expectations may help. Do set expectations on other people!
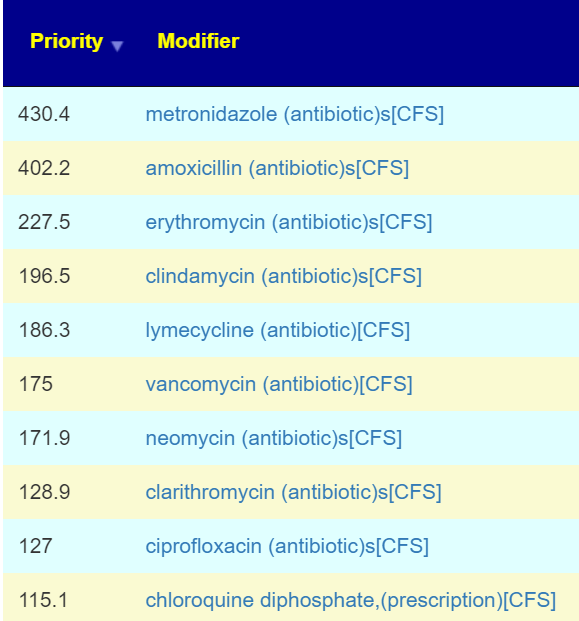
- Microbiome Analysis and changing diet to better normalize. The microbiome appears to influence anxiety greatly. Also Gut bacteria linked to personality[2020]
- DNA testing — technically it could help, but still early days for research. The one exception is testing for inherited genetic coagulation factors.
Needless to say, I favor microbiome manipulation greatly — because it is the easiest factor to address (can be hard to give up favorite unhealthy foods).