This uBiome was different than others — age may be a factor dealing with microbiome shifts in CFS.
Short History of Key Points
- Original Onset appear to have been triggered by an amalgam being removed in grade 12
- Subsequent was sinus infection etc with likely an inappropriate antibiotics for this person
- Repeat when the amalgam was replaced again a year later
- At university, the dorm he was in appear to have had significant mold issue
- fresh fruit would go moldy in 1-2 days constantly
- room mate with autoimmune issues was having constant flares
- Today, he is back at university in a different dorm (does not appear to have mold issues)
- Has been doing variety of herbs etc that been suggested on this blog over this year
- Greatly improved compared to the last few years
- No stomach or digestive issues at present
- This uBiome was done in the last few weeks (his current state)
“Interestingly enough, I’ve also had a higher precedence of cavities since college started and they only got worse when my symptoms of fatigue began as well”
Current Status
Unlike most CFS patients, the ratio of Firmicutes to Bacteroidetes was close to normal.
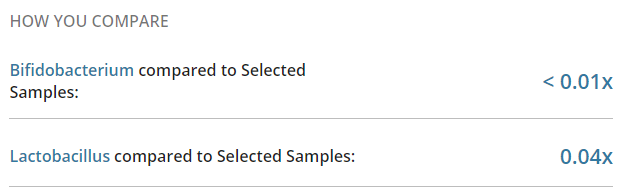
- Bifidobacterium was 61% of normal
- Lactobacillus was < 1% of normal
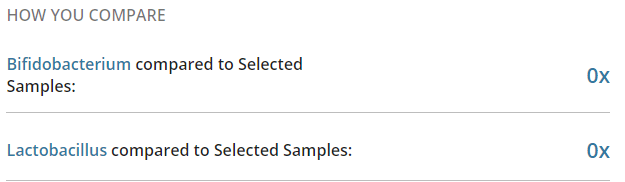
- Akkermansia – none reported.
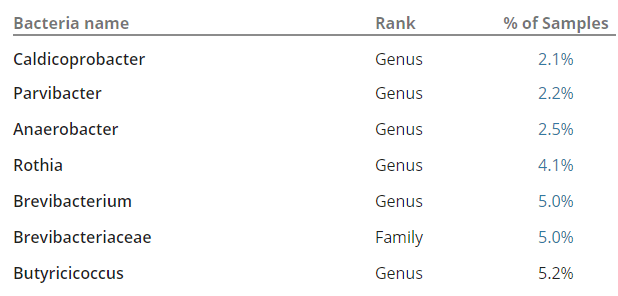
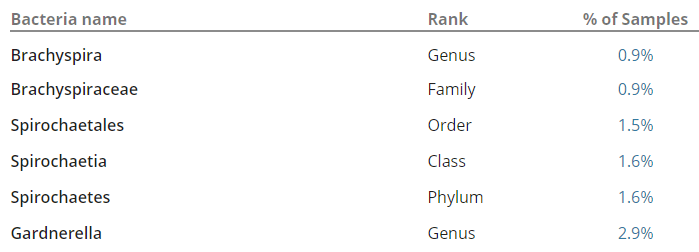
At the Genus level, there were several abnormal high:
- Collinsella: 263% of normal (high seen in 25%)
- Enterorhabdus: 326% of normal (only rarely seen)
- Intestinibacter: 241% of normal (high seen in ~50%)
- Roseburia: 247% of normal (high seen in 30%)
What do we find:
- Collinsella and Enterorhabdus are reduced with smokers with Crohn’s Disease [2016]
- “A lower abundance of Roseburia has been observed in patients suffering from inflammatory bowel disease.” [ubiome]
- Higher level seen with diets with whole grain [2013]
- Metformin will “increases Escherichia and lowers Intestinibacter abundance” [2015]
- “elevated levels of Roseburia may be associated with weight loss and reduced glucose intolerance.” [ubiome]
Pre-diabetic?
Looking at some articles, there is a possibility that being pre-diabetic may be a factor (hint: testing should be considered). A pre-diabetic diet should be consider – see this WebMD page. Diabetes does run in his family.
Analysis
This reader abnormalities do not have any association with IBD etc. His values were high when a low value was associated. The uBiome agrees with his symptoms.
I was at my dentist recently and she gave me a list of supplements that help with dental gum health (will do a post on this) which almost looks like it was written for CFS patients — the same items occur constantly. One of my own crowns is a concern to her because the x-rays are unclear if I have grown a colony of bacteria under the crown (a location very hard to treat with antibiotics, but also a location which could re-infect the body). She was recommending removing the crown and send samples for analysis.
For amalgams, the traditional view has been the mercury has created health issues. There is an alternative explanation, the area under the amalgam may be an ideal colony site for some types of bacteria; bacteria that could be release slowly or in quantity when dental works occurs. This reader appear to have suffered multiple insults: Amalgam-bacteria onset, antibiotics that further shifted his microbiome, prolonged mold exposure adding more shifting of his microbiome. He is getting his mouth into better shape, he found brushing with Alpha-Lipotic Acid helped his mouth(I love readers sharing successful experiments!) . His mouth appears to be a key source for his CFS.
Fortunately, he appears by symptoms and ubiome to be on his way to recovery.
Bottom Line
My usual criteria for probable CFS using uBiome is having two of the following three very low:
- Bifidobacterium
- Lactobacillus
- Akkermansia
This uBiome made that criteria but not in the usual way. He appears to be on the way to recovery (but need to be wary of factors that could cause flares or worst)
- The glucose/diabetes related issues hints that Lactobacillus Fermentum ME-3 should be tried. [2014][2016]
- Consider breaking a capsule apart and leave the contents in your mouth for a while after brushing your teeth
- You may wish to try this with other probiotics.
- The chewing of various natural gums (myrrh, mastic, boswellia) should also be considered because of the dental issues (and the potential of the mouth being a reserve to re-introduce bacteria into the guts).
- Do a variety of oral probiotics
- Do appropriate herbal teas: Triphala, Neem, etc — we want their contents to hang out in your mouth area.
- Redo uBiome in December to see what shifts has occurred
As always, consult with a knowledgeable medical professional before adding or changing supplements.