I often have read on the web that there is no test for CFS. This is very incorrect — there is no official test for CFS nicely bundled up. “No current diagnostic tool or method has been adequately tested to identify patients when diagnostic uncertainty exists.”[2014] What we find in the literature are many tests available to confirm CFS/ME when symptoms presents.
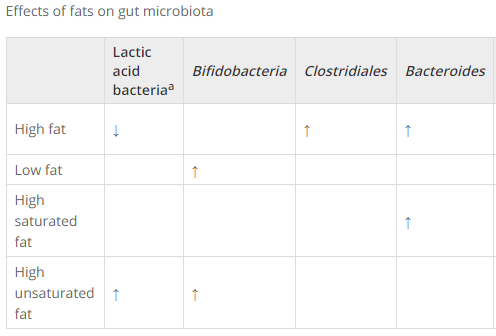
This post reviews where there have been a strong association of abnormal laboratory results to CFS/ME patients. These tests can often be used to confirm that the diagnosis is correct. For example: is TGF-β elevated and resistin lower? etc. In terms of microbiome results from uBiome.com: low or no lactobacillus, low or no bifidobacteria, low or no akkermansia muciniphila, low or no E.Coli.
- Cytokine signature associated with disease severity in chronic fatigue syndrome patients[2017].
- ” Seventeen cytokines had a statistically significant upward linear trend that correlated with ME/CFS severity: CCL11 (Eotaxin-1), CXCL1 (GROα), CXCL10 (IP-10), IFN-γ, IL-4, IL-5, IL-7, IL-12p70, IL-13, IL-17F, leptin, G-CSF, GM-CSF, LIF, NGF, SCF, and TGF-α. Of the 17 cytokines that correlated with severity, 13 are proinflammatory, likely contributing to many of the symptoms experienced by patients and establishing a strong immune system component of the disease. Only CXCL9 (MIG) inversely correlated with fatigue duration.”
- “On average, TGF-β was elevated (P = 0.0052) and resistin was lower (P = 0.0052) in patients compared with controls. “
-
- Another study about to be published….
- A diagnostic biomarker profile for fibromyalgia syndrome based on an NMR metabolomics study of selected patients and controls[2017].
- “an algorithm for the diagnosis of FMS consisting of three metabolites – succinic acid, taurine and creatine – that have a good level of diagnostic accuracy … analytically detectable within their urine”

- “Finally, the involvement of gut microbial–host metabolic perturbations in FMS may prove to contribute significantly in defining the clinical profile in FMS.”
- “an algorithm for the diagnosis of FMS consisting of three metabolites – succinic acid, taurine and creatine – that have a good level of diagnostic accuracy … analytically detectable within their urine”
- Index markers of chronic fatigue syndrome with dysfunction of TCA and urea cycles[2016].
- ” The combination of ornithine/citrulline and pyruvate/isocitrate ratios discriminated CFS patients from healthy controls, …These findings provide compelling evidence that a clinical diagnostic tool could be developed for CFS based on the ratios of metabolites in plasma.”
- Reduced diversity and altered composition of the gut microbiome in individuals with myalgic encephalomyelitis/chronic fatigue syndrome [2016].
- “the data obtained from 16S rRNA and inflammatory markers, individuals were classified correctly as ME/CFS with a cross-validation accuracy of 82.93 %.”
- MicroRNAs hsa-miR-99b, hsa-miR-330, hsa-miR-126 and hsa-miR-30c: Potential Diagnostic Biomarkers in Natural Killer (NK) Cells of Patients with Chronic Fatigue Syndrome (CFS)/ Myalgic Encephalomyelitis (ME) [2016].
- Mitochondrial DNA variants correlate with symptoms in myalgic encephalomyelitis/chronic fatigue syndrome[2016].
- “Analysis of mitochondrial genomes in ME/CFS cases indicates that individuals of a certain haplogroup or carrying specific SNPs are more likely to exhibit certain neurological, inflammatory, and/or gastrointestinal symptoms. “
- “No ME/CFS subject exhibited known disease-causing mtDNA mutations. Extent of heteroplasmy was low in all subjects. Although no association between mtDNA SNPs and ME/CFS vs. healthy status was observed, haplogroups J, U and H as well as eight SNPs in ME/CFS cases were significantly associated with individual symptoms, symptom clusters, or symptom severity.”
- Myalgic Encephalomyelitis: Symptoms and Biomarkers [2015].
- Longitudinal analysis of immune abnormalities in varying severities of Chronic Fatigue Syndrome/Myalgic Encephalomyelitis patients [2015].
- “Over time, iNKT CD62L expression significantly increased in moderate CFS/ME patients and CD56(bright) NK receptors differed in severe CFS/ME. Naïve CD8(+)T cells, CD8(-)CD4(-) and CD56(-)CD16(-) iNKT phenotypes, γδ2T cells and effector memory subsets were significantly increased in severe CFS/ME patients at 6 months. Severe CFS/ME patients were significantly reduced in CD56(bright)CD16(dim) NKG2D, CD56(dim)CD16(-) KIR2DL2/DL3, CD94(-)CD11a(-) γδ1T cells and CD62L(+)CD11a(-) γδ1T cells at 6 months.”
- Biomarkers for chronic fatigue [2012].
- Use of single-nucleotide polymorphisms (SNPs) to distinguish gene expression subtypes of chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) [2014].
- “This study provides evidence that human SNPs located within CFS/ME associated genes are associated with particular genomic subtypes of CFS/ME.”
- “Microbial infections in eight genomic subtypes of chronic fatigue syndrome/myalgic encephalomyelitis. [2009]”
- “In patients with CFS/ME, differential expression was confirmed for all 88 genes. Q-CFS/ME had similar patterns of gene expression to idiopathic CFS/ME. “
My Own Favorite Ad-Hoc Markers
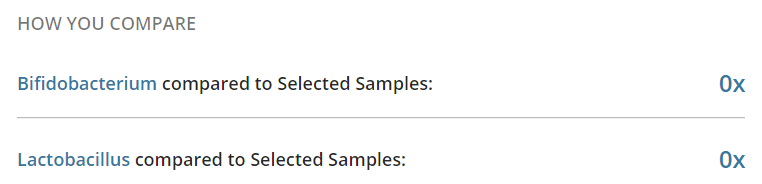
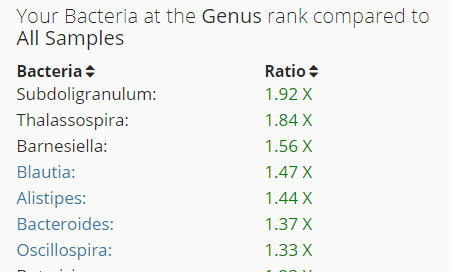
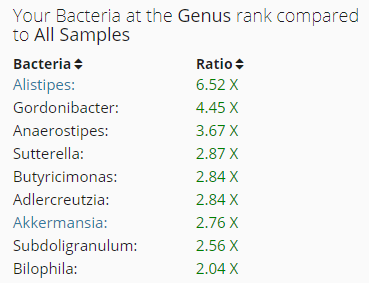
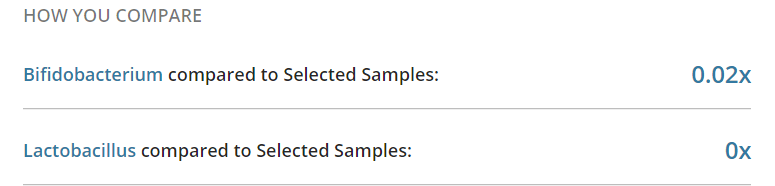
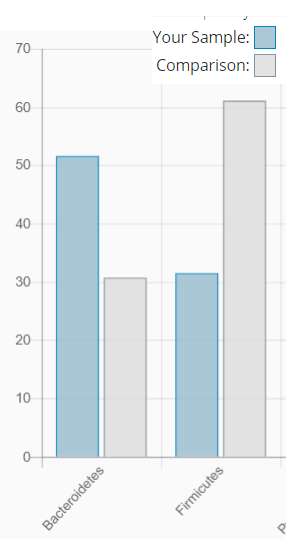
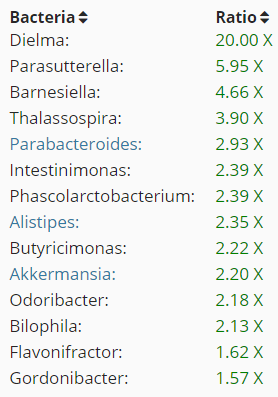
From uBiome:
- Low or no Lactobacillus
- Low or no Bifidobacteria
- Low or no E.Coli
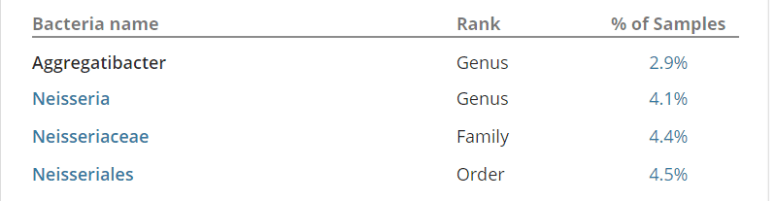
- Not directly reported, but it parent is: Enterobacteriaceae which will be NOT listed in results, or at something like 2% of the reference group
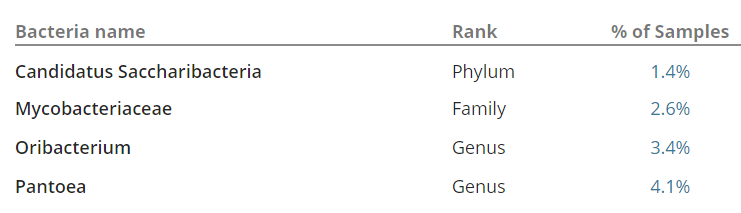
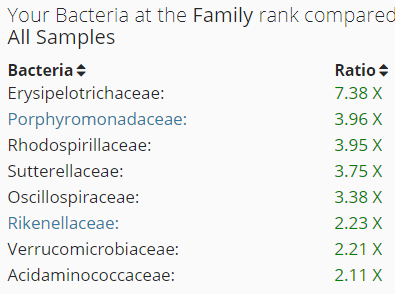
- Low or High Akkermansia (parent is Verrucomicrobiaceae)
Bottom Line
Yes, there is testing that can be used to increase the certainty of a CFS/ME diagnosis (or exclude it — which should lead to further testing).