A reader forward me a link to “Find the cause of fibromyalgia” article (Spanish) which states:
- “Thanks to a study carried out with 3,000 people – of which two thirds of them were affected by fibromyalgia and chronic fatigue – it has been possible to determine that there are 90 polymorphisms in the DNA of the patients that affect the nervous and nervous system.” I have a few of them listed in this 2016 post.
The problem with DNA causing FM/IBS/FM etc, it the tendency towards resignation (“It’s in my DNA — how can we fix it!!!”). This is very wrong, a very important concept to remember is epigenetics – “In simplified terms, epigenetics is the study of biological mechanisms that will switch genes on and off.”[A Super Brief and Basic Explanation of Epigenetics for Total Beginners]. The key factors of turning genes on and off are items like stress and diet (including availability of minerals, amino acid etc – often a by product of the microbiome).
Microbiome is also inherited in two ways
“microbes (and their genetic material, collectively known as the microbiome) within the body can influence all kinds of traits as disparate as digestion and behavior, and can be passed down to offspring, he says. Just like a person’s own DNA.” [Newsweek]
“A genome-wide association analysis of over 1,000 twins in the UK supports that some parts of our microbiomes are inherited and shaped–not through a spread of microbes from parent to child, but through our genes. The results, revealing new examples of heritable bacterial species–including those related to diet preference, metabolism, and immune defense — appear May 11 in Cell Host & Microbe‘s special issue on the “Genetics and Epigenetics of Host-Microbe Interactions….The investigators used the genome-wide association approach to look for connections between genetic variations between twin pairs and certain bacterial types that were present and stable in the study subjects.” [Science Daily] So DNA impacts the microbiome … but the microbiome is much more changeable than DNA!
Model
- “Events” trigger DNA to turn some FM/IBS/CFS genes ON (epigenetics)
- Same event to someone else with different DNA has no problems.
- The change of genes may also result in alteration of the microbiome
Model prediction
- Create an epigenetic event by altering microbiome, supplements.
- Epigenetic events shuts down the genes.
- Remission (NOT cure).
Bottom Line
There is no defined universal protocol possible for CFS/FM etc. We have at least 80 SNPs for FM, likely a similar number for IBS, CFS etc. Each person has some combination (not all of them), which supported the epigenetic change/microbiome change. The microbiome changes are likely even more complex.
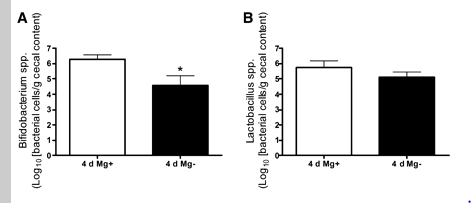
There are commonality that most patients have in common. You may be high in one bacterial genus and the CFS person next to you may be low in the same genus. What is common are low lactobacillus, low bifidobacterium, low in typical E.Coli (possibly high in atypical E.Coli), low in typical Enterococcus (possibly high in atypical Enterococcus).
With this complex situation, we have very little research, extremely few tools, and the tools tend to be crude. In one way we have a big box of nuts and bolts in front of us and a bunch of metal connectors with different size holes in them. Some nuts and bolts are metric and some are SAE. This does not mean we are helpless — it means we need to be patient to find the right nut to match with the right bolt and then find the right metal connector where it is a tight fit. There is no handy IKEA assembly manual with all of the parts nicely bagged.
The stuff goes together if we approach it in an organized manner. Take one nut at a time, try different bolts until you have some possible matches. If frustrated, go on to the next nut (or bolt).
What are these nuts, bolts and connectors — herbs, spices, supplements, probiotics and antibiotics. Not all will be needed by everyone. Trying too hard to fit a nut to a bolt may end up jamming it.