Some early feedback has resulted in my adding a new page. This is providing more detail on this earlier post. On the Analysis page (where you are sent once a sample is selected), you will see a new link, shown below:
Clicking on this will take you to a page showing the 10 most atypical bacteria (all levels), as shown below. Three examples — all for the same person over 3 years. With the new algorithm, too low is rarely seen.
Clicking on the name will take you to the reference library so you can see the known information about each. This allows you to custom build your suggestions (instead of automatic suggestions).
Determining what is or is not a significant shift in the microbiome is challenging. My original algorithm on http://microbiomeprescription.com/ was based on reverse engineering the normative values that uBiome appear to be working from. This was a quick and dirty solution — what was possible a year ago. Doing some R analysis of the contributed microbiomes and rethinking the issue of determining what is atypical, I borrow some algorithms/observations from a work project whose goal was to detect abnormal behavior of computer systems.
Both microbiomes and complex computer system tend to share similar challenges: they are not normal distributions and often long tailed (skewed) which means that averages and standard deviation often produce poor results for detecting abnormal values.
We will Box Up the Issue!
A common process in filtering data for machine learning etc, is excluding outliers. We are actually interested in finding the outliers! This is often done by boxplots. An example of some of phylum level bacteria is shown below. (Note 1.0 = 100%)
outliers are the round circles
And we can do it to lower levels, for example, order
Down to Species
The solid black line is the median (almost an average). For B.Vulgatus we see that the range of values from 25%ile to median is almost the same as median to 75%ile. For B. uniformis, this is very different.
New Algorithm looks for these outliers and only deem these to be significant. For a post showing more details, click here.
What is the main difference?
I put several samples thru comparing the NUMBER of bacteria shifts deemed significant. The first number is with the old algorithm, the second number is with this new algorithm.
181 -> 55
193 -> 56
160 -> 43
133 -> 33
133 -> 29
In theory this means that we are much more focus on the major shifts and not any shift. You can see the number of items identified on the suggestion page.
Clustering is bunching observations (people’s microbiome) into groups based on similarity. In english, we want to see if one people with shift in one type of bacteria also have a shift with a different type.
After this we scale the data and proceed to explore.
First a Box Plot
This shows the odds of outliers (data is scaled remember). We see Bacteroidetes are well behaved (normal distribution), but phylums like Actinobacteria, Verrucomicrobia, Proteobacteria, and Firmicutes have atypical behavior.
Bacteroidetes vs Firmicutes
These are the dominant two phylum. When we plot the data we see a clear ‘trade off’ pattern between them. We also see that there is a number where Bacteriodetes < 0.1 (scaled).
Filtering to these low ones (86), removing the sampleId column, and searching for number of clusters that would classify these many observations, we see that there an ‘elbow’ at 3
Applying a dendrogram, we see that these 86 people fall into some distinct groups.
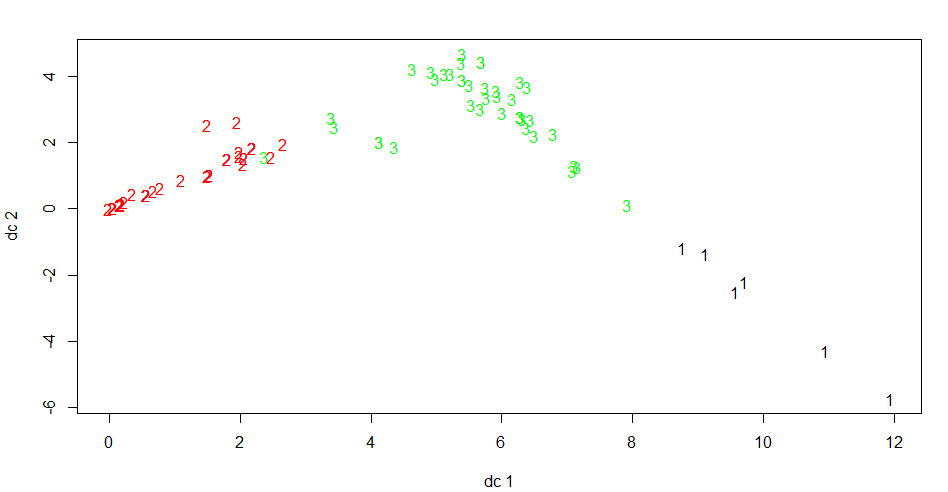
Plotting the cluster illustrates that we have good separation.
Looking at the averages by phylum for each of the groups we see some clear patterns:
We originally filter to Bacteroidetes < 0.1, but we see that this group could be divided into very very low (Groups 1 +2) and low (3).
Returning to other Phylum
Three plots are shown below — Actinobacteria, Verrucomicrobia, Proteobacteria
Odd line is seen below — almost a straight inverse line for one set of data
Homework
My purpose is to get people exploring the data. If you look at Data Science: Tax Rank and Symptoms, you can find the sampleIds with symptoms (a subset of the data above). The assignment is simple — can you find any symptoms that appear to be associated with the clusters you may have found?
You may wish to pre-filter to only the phylum with symptoms… and then cluster.
The results were not surprising for me — because the focus was on a single drug.
Overall response rates were 35.1% in the placebo group and 26.0% in the rituximab group (difference, 9.2 percentage points [95% CI, -5.5 to 23.3 percentage points]; P = 0.22). The treatment groups did not differ in fatigue score over 24 months (difference in average score, 0.02 [CI, -0.27 to 0.31]; P = 0.80) or any of the secondary end points. Twenty patients (26.0%) in the rituximab group and 14 (18.9%) in the placebo group had serious adverse events.
The Rituximab saga began in 2004 when two oncologists noticed that Rituximab – a B-cell depleting drug often used in cancer – not only cured one of their patient’s cancer but eliminated their chronic fatigue syndrome (ME/CFS) as well. After two more ME/CFS patients responded similarly, they began their work on ME/CFS in earnest.
I have personally met two people with CFS that had cancer — and the CFS disappeared with the cancer treatment (usually included chemotherapy).
Cancer+CFS is not a CFS microbiome
A search on pub med for cancer and microbiome returns over 4400 studies. Cancer causes a change of the microbiome — yes, it may still be dysfunctional but it is dysfunctional in another way. The full cancer treatment protocol appears to reset the microbiome (likey by devastating it).
Chemotherapy and radiotherapy treatment regimens for gastrointestinal, peritoneal and pelvic tumours can disrupt the intestinal microbiomeand intestinal epithelia. Such disturbances can provoke symptoms such as diarrhoea, nausea and vomiting. Chemotherapy and radiotherapy induced gastrointestinal toxicity aggravating intestinal microbiome dysbiosis is postulated to adversely alter the intestinal microbiome, with a consequent induced pro-inflammatory effect that disrupts the intestinal microbiome-epithelia-mucosal immunity axis.
A reader asked for more details, so I thought that would do a short listing of some major ones — oh, almost all of these have known microbiome shifts associated with them. Personally, I have two of the items listed, Autism Spectrum and ME/CFS.
Source: US Government Job Accommodation Network looking at conditions with stress intolerance as being potential accommodations by employers
Often the information (including from HR) is just a ” For this reason, employers may need to look for ways to reduce stress and/or remove stressors in the work environment. ” , often with no serious examples of what could be done.
Stress Org lists some of the main sources of stress:
I know that I work in an industry that is often deemed to be high stress, Information Technology — yet for most of my 4 decades, there have been actually little stress: I have had boss that respected my opinion, gave me the resources or time table that I asked for … and I just done what was asked of me.
Problems do occur in IT with people who are ‘full of themselves’, that is, they believe they can walk on water! (I usually wait for a cold winter north of 60 degrees before I walk thpath). My own issues have usually been with managers that believe that the way to get people to work hard is to keep them in a state of crisis and/or under pressure! Wilful stress. When confronted by HR request to produce a low stress environment — they are clueless and will blow off the request as “that’s the nature of this business”. It’s not. It is the nature of all businesses where people are promoted to managers may never have done a single sociology or psychology of business course.
For my first management role in business some 40 years ago, there was 3 months of courses over the first year to insure consistency of management practise. It is little wonder that the Harvard Business Review found that picking a person at random to be a manager perform as well as a carefully interviewed candidate!
One of my favorite bosses said: A good manager is someone that reduces (or hides) uncertainty and stress coming from above from those reporting to him.