A reader asked me to review their microbiome and test results, for items to discuss with their medical professional. As always this is not advising what to do; suggestions should always be reviewed by your medical before implementing.
The Person
This woman developed CFS around Lake Tahoe in 1987. Lyme and Mold issues.
- Adverse effects from:
- vancomycin (linked to bacteria it modifies)
- xifaxan (Rifaximin) (linked to bacteria it modifies) Nov 2019
- Resulting in MD prescribed Iron supplements, resulting in
- 23 lb gain (heaviest ever!) (fat gain)
- High cortisol,
- Insulin resistance,
- Bloating
- Antifungals and antibacterial herbs for the past 3 years for mold and Lyme. history of off and on antibiotics for Lyme and coinfections for decades etc.
- Cytomegalovirus and Epstein Barr (common with ME/CFS)
- Tried resistant starch(oatmeal and green banana) and my bad microbes tripled (unclear which ones were deemed bad)
- Gluten-free for years
- Food poisoning 5 years ago
- Feels hypoxic (low oxygen to brain) – likely caused by Protein S deficiency that is part of the coagulation change (according to tests)
- Genetic issues processing phenylene, leucine and lysine. And also oxalate issues
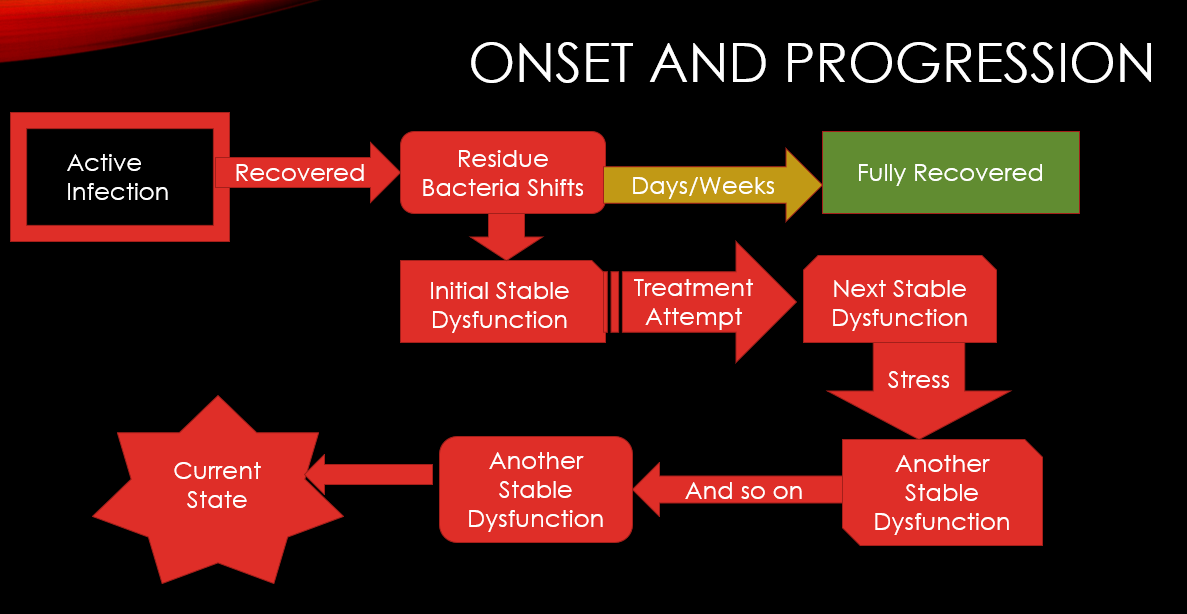
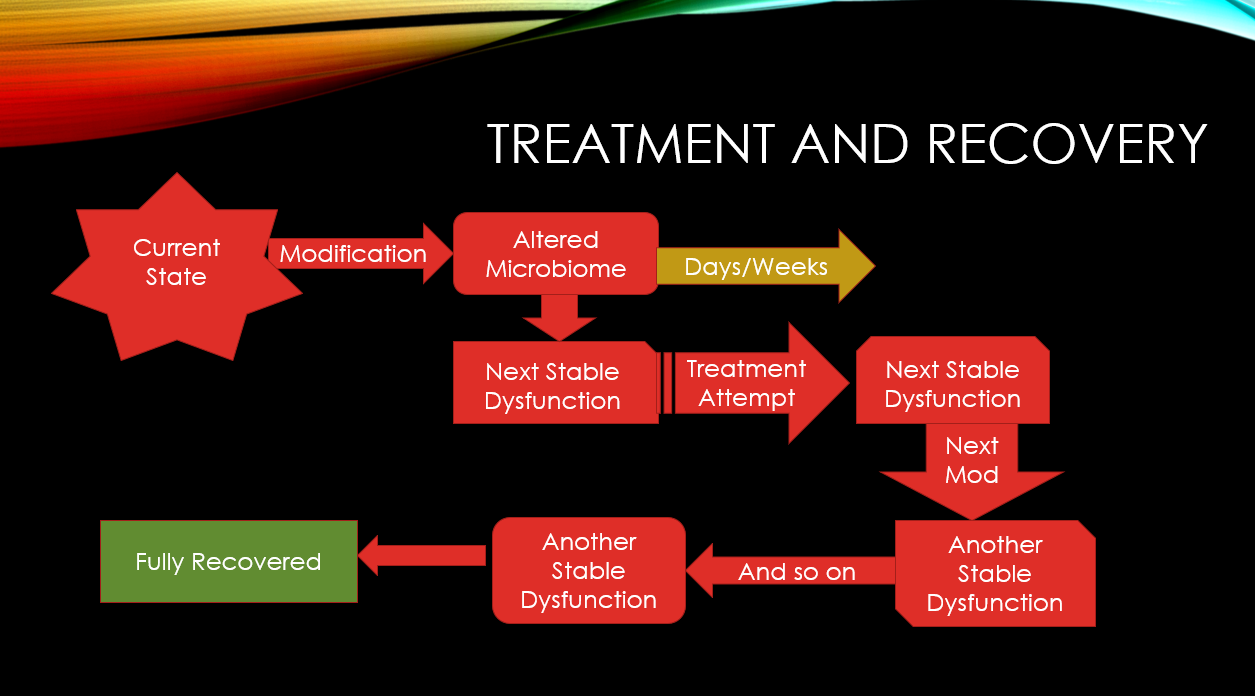
Markov Cascade Model
This chart shows how overtime the microbiome can recover or continue to cascade (evolve). It is not a one step change, it’s a series of changes over time caused by diet, treatment attempts, age etc. This is essential to understand why things change and that it is not a one-step recovery.
The Samples
We have five samples from Dec 2020 until May 2021. Multiple samples is a short period of time allows the daily variation to be minimize. Due to age, we do not have to be concerned with time in cycle impacting her microbiome (a key factor for females doing comparison samples)
Initial Notes
Going to comparing multiple samples, I walked thru each of the outliers and jolt down concerns

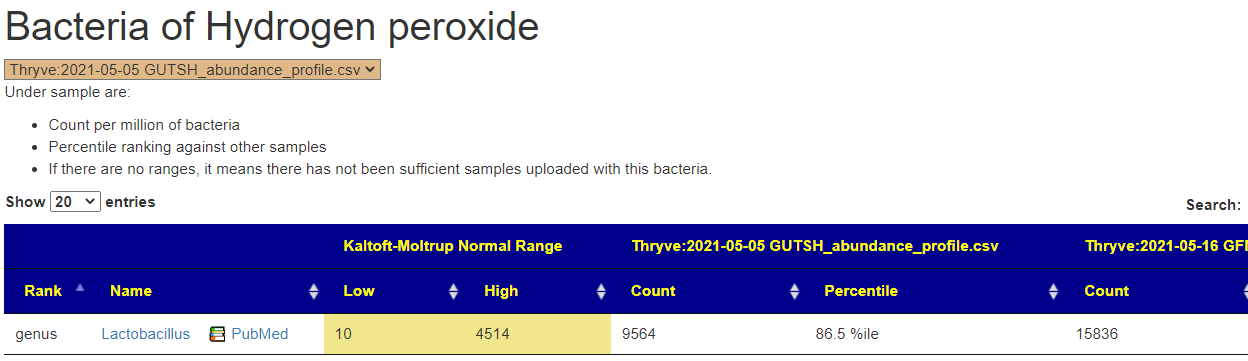
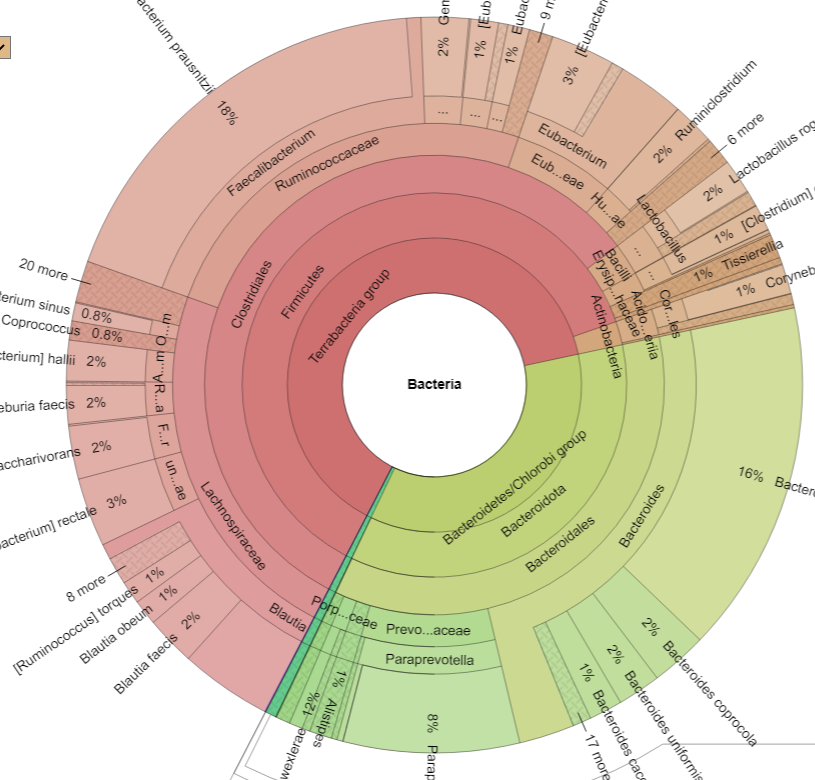
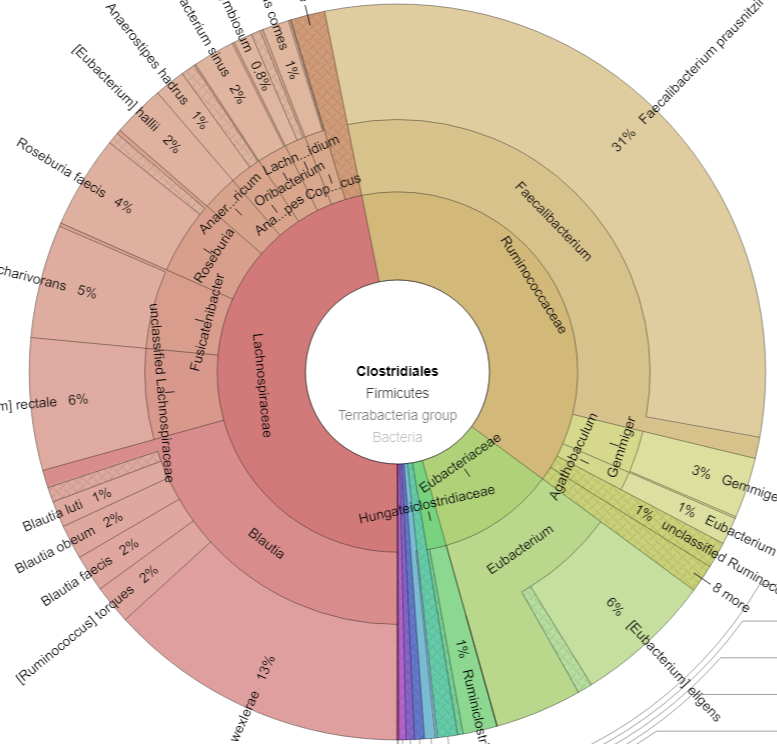
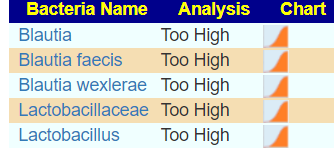
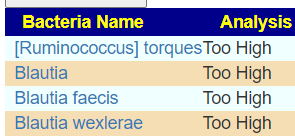
- Bacteria
There are a few more, but we should call out that one species of a genus(Blautia) is very high and another is very low.
- End Products: the low level of gluten consumers hints that a gluten-free diet should be tried.
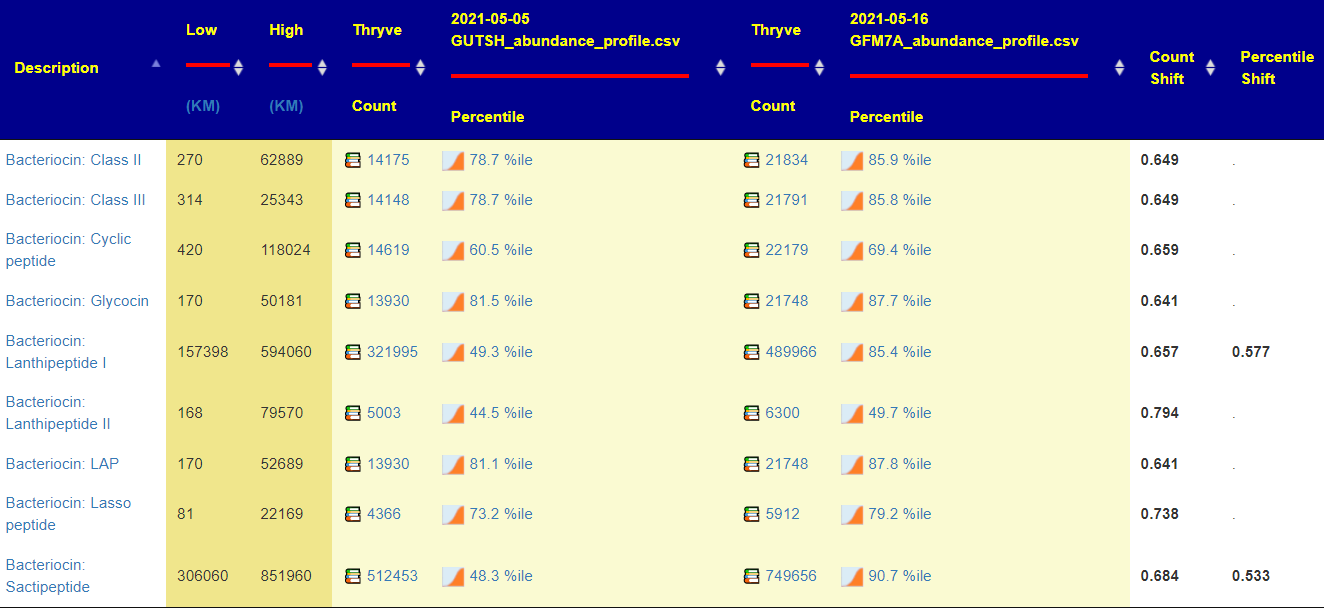
- KEGG Bacteria Products
- All of the items connected with iron (ferro… – seven of them) had low warnings, suggesting limited ability to handle iron
- High
- protocatechuate
- protein L-glutamate – consistent with diagnosis GABA and Glutamate in Fibromyalgia and Chronic Fatigue Syndrome
- MnIVO2 (O2Mn)
- mesaconate
- methanofuran
- Mn3+ (Manganese)
- KEGG Enzymes – a wall of alerts, nothing special spotted
- KEGG Module
- Low
- (M00009) Citrate cycle (TCA cycle, Krebs cycle)
- (M00011) Citrate cycle, second carbon oxidation, 2-oxoglutarate => oxaloacetate
- (M00063) CMP-KDO biosynthesis
- (M00855) Glycogen degradation, glycogen => glucose-6P
- (M00535) Isoleucine biosynthesis, pyruvate => 2-oxobutanoate
- and many more. No consistent highs
- Low
- Medical Condition (PubMed)
- No matches – this may indicate that the person has moved outside of the typical ranges
Building Suggestions
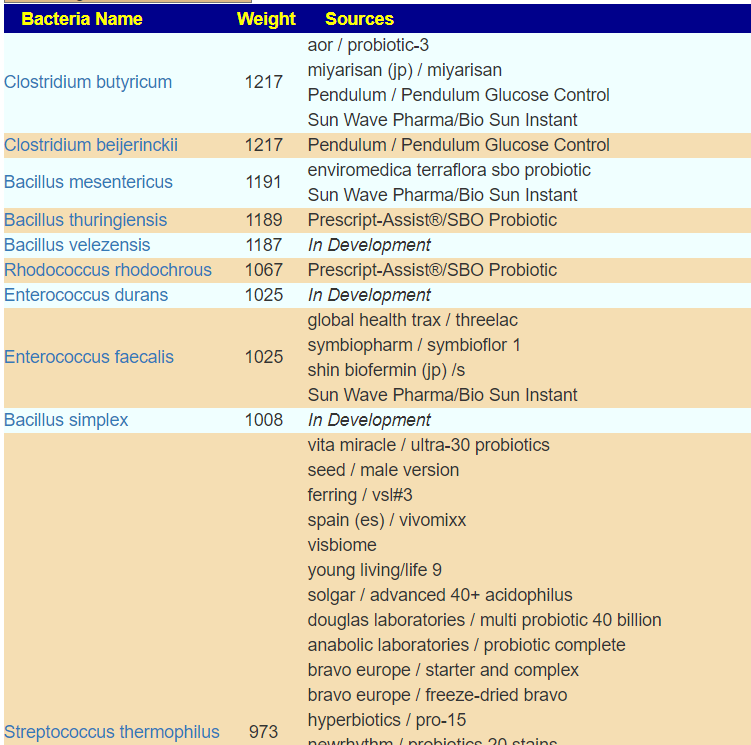
The numbers for the recommendations are among the highest that I have seen!!! This implies taht a lot of enzymes are not being produced. I would suggest the three easiest to obtain for a start, single Species with research (as shown below with the Books emoji)
- Miyarisan (Clostridium butyricum), Clostridium Butyricum MIYAIRI 📚
- symbiopharm / symbioflor 1 or shin biofermin (jp) /s (Enterococcus faecalis),
- Custom Probiotics (Streptococcus thermophilus) Streptococcus thermophilus ST-21 📚
For dosages, start low and slowly increase to the common therapeutic dosages
KEGG supplement list is long, even when reduced to just 3%ile
- Amylase (Enzyme)
- beta-alanine
- D-Ribose
- Glycine
- L-Cysteine
- L-glutamine
- L-Histidine
- L-Lysine
- L-methionine
- L-Serine
- NADH
- Selenocysteine
Prior to suggesting any of this list, i want to look at advance suggestions. The options that I picked
First, out of curiosity, given the experience with antibiotics, I looked at only antibiotics. Only a few of several hundred in the database made it on the possible list and at low confidence. The top 3 are often suggested with ME/CFS patients. the avoid list is massive. My impression is no antibiotics, but we need to confirm other paths are more probable to help.

I played with the other prescription options and the results were similar. So returning to the default suggestions we end up with an interesting list of do and don’ts

What makes it interesting is that a lot of to avoid are common suggestions from MDs treating ME/CFS with one-recipe fits all for ME/CFS. For example
- Avoid all B-vitamins
- No vitamin C
- No Melatonin
- No quercetin
- Avoid Lactobacillus probiotics and likely bifidibacterium
The top item to avoid is luteolin. The foods that contain it are listed here and include celery seed, thyme, parsley, peppermint, rosemary and olives.
On the plus side I see my favorite ‘antibiotics herb’ being listed, triphala. Changing the diet to resistant starches and away from high gluten food. Care must be taken to make sure you do not destroy the resistant starch as shown below:

Using Resistant Starch Content in Foods Commonly Consumed in the United States: A Narrative Review [2020], we see that Lima (butter) beans and Kidney beans should become part of your regular diet.
Antibiotics for Fusobacterium
The reader is interested in antibiotics for fusobacterium. I usually try to discourage single-bacteria focus because side-effects on other bacteria may make the person worse. Often this approach leads to frustrations because things “did not work“.
We start by looking at the antibiotics (this link) where we find 103 different antibiotics that reduces it. Just below this section of the page we also see the bacteria that encourages or discourage; for her latest sample, none of these appear to be in play.
Looking at the suggestions for antibiotics only, and turning all the  Show links to studies used for suggestions and setting the number of suggestions high, we see all antibiotics with probable positive impact, we end up with this list only.
Show links to studies used for suggestions and setting the number of suggestions high, we see all antibiotics with probable positive impact, we end up with this list only.

We then click each link to see what each suggestion actually modifies, on #2, we encounter success. It reduces this bacteria AND increases a different bacteria in the wrong direction (Pediococus is TOO high). This illustrates the challenge of being focused on one bacteria.

Remember that we balance good and bad impact — so remember to check each items
There is no option to model what will probably happen. My goal is to increase the probability of a suggestion being helpful. This is a decision that the medical professional needs to make (ideally after being made aware of side-effects).
Bottom Line
This person is not the usual pattern with pretty extreme shifts in the microbiome. My suggestion for a course of action to discuss with your medical professional would be
- reduce/eliminate any supplements/drugs not listed above for a month
- shift over to the diet style above, with the few probiotics suggested
- start at a low dosage of Triphala (we buy it organic bulk and make our own capsules) and increase it slowly to at least 2 grams/day, ideally 8 grams/day [basis of dosages]
To me the key thing is to simplify the influences on the gut and allow it to stabilize and then proceed from there with changes followed by re-test and a new set of changes.