Today I got hit with a bunch of ads on Facebook for the above. I see that some of the ads are targeted for irritable bowel syndrome (IBS). My first impression is what is it? Has it been demonstrated to help anything (besides the pocket book of promoters)? What is the probable monthly cost of an effective dosage? This post attempts to answer these questions. Similar posts from the back:
The aim of this paper is therefore to critically review the current literature surrounding the use of BPC 157, as a feasible therapy for healing and functional restoration of soft tissue damage, with a focus on tendon, ligament and skeletal muscle healing. Currently, all studies investigating BPC 157 have demonstrated consistently positive and prompt healing effects for various injury types, both traumatic and systemic and for a plethora of soft tissues. However, to date, the majority of studies have been performed on small rodent models and the efficacy of BPC 157 is yet to be confirmed in humans.
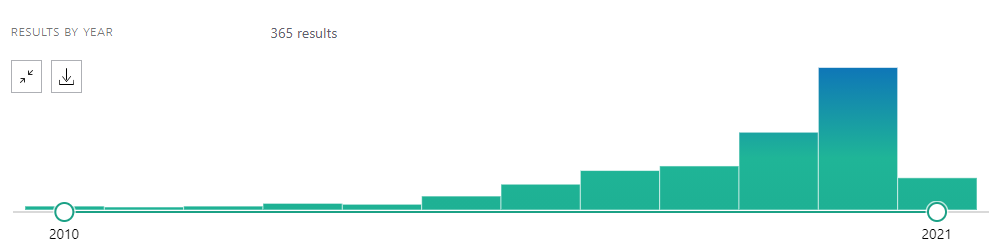
The first question is simple, should be expect it to be confirmed in humans? The longer it has been since discovery, the higher the probability. IMHO 5-7 years is a reasonable expectation. Turning to PubMed, we see it has been written about for thirty years.
What is it?
Pentadecapeptide BPC 157, composed of 15 amino acids, is a partial sequence of body protection compound (BPC) that is discovered in and isolated from human gastric juice. Experimentally it has been demonstrated to accelerate the healing of many different wounds, including transected rat Achilles tendon.
The version being sold is patented, older versions do not survive stomach acid etc. The patent gives the sequence of these amino acids is given in the patent, “pentadecapeptide (abbr. BPC-157 or bepecin) having an amino acid sequence: Gly Glu Pro Pro Pro Gly Lys Pro Ala Asp Asp Ala Gly Leu Val “
The FDA has issued warnings about it. From unsafe manufacturing [2018], as well as other agencies
While the peptide BPC-157 is not presently included on the World Anti-Doping Agency (WADA) Prohibited List, it is important for athletes to be aware that this substance is not approved for human clinical use by any global regulatory authority, it may lead to negative health effects, and it could be added to the Prohibited List at any time based on new research. A
There is a clinical study from 2015 that I found PCO-02 – Safety and Pharmacokinetics Trial The high dosage was 8-24 mg/day. Thus the above bottle is enough for 4 days, so about $450/month. There has been no update of this trial for 7 years. Usually, no update means no positive results (99% of the time)….
Bottom Line
There is no trustworthy evidence that it helps, it has a high cost (when purchased from the promoters) and lack FDA approval (it is being sold as an unregulated supplement). The price being asked is CRAZY! Some sources are selling it in bulk for as low as $3/kilogram! So BEWARE and save your money!
I view Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) — and many other conditions– as being either a pure microbiome dysfunction, or a microbiome dysfunction that contributes significantly to many of the symptoms. If you walk into your typical medical office and ask questions about this you will likely be met with a variety of responses (depending on their psychology) that are not helpful.
A reader asked “Why is this?” The easiest way to understand the issue is to look at the number of studies on pubmed about the microbiome
What does this translate to? Unless your MD finished his studies in the last 5 years, there is very little chance that there was any significant coverage of the microbiome in courses. Yes, they took microbiology — the study of bacteria; but the microbiome is different. How so?
Microbiology can be compared to understanding how a person‘s psychology changes as they ages from a child, to an adult, to an elderly. The microbiome is understand sociology of people in a society. The microbiome is the understanding of interactions and interplays. It is more complex. Far more complex.
This is why MDs and naturopaths tend to look for the single bacteria or virus responsible. That is precisely what they had training in, the comfort principle of medicine.
A second factor is simple, specialization. “Ah, the microbiome belongs to the human gastrointestinal system, so the patient should be referred to a gastroenterologist!” Wait! they treat very specific diseases only and not items like a diabetic’s microbiome. Tossing patients to specialists is a common practise — the problem is that there are rarely specialists in this area. It’s my least favorite game: PPP – “Patient Ping Pong”.
Old techniques versus Best techniques
Often old techniques could be rephrased as ‘current accepted best practises’. In my Uni days, I has several professors tell me “Do not go into Engineering or Medicine, you are brilliant — but you are also creative and innovative, that will end your career in those areas”. I have an additional characteristics, I am a high functioning ASD person. Why is that important? It means that I tend to ignore social pressure and conformity; instead, I march to my own drum beat along whatever path looks interesting (and have little anxiety about stepping off existing paths). Back to the topic….
What is the best technique for dealing with the microbiome? It is simple, use various types of artificial intelligence and machine learning. The problem with this for MDs is that machines are giving them advice that they are incapable of understanding the why. It is not that the MD is dumb, it is because the problem is very very complex.
One type of machine learning is called “Random Forest“. I have used them professionally when I worked for Amazon. Microbiome studies started using this in 2010 and the number of studies are exploding yearly — why, because it works!
The problem is that this is a new discipline called data science, an specialized application of advanced statistics. Yes, MDs and medical researchers often did a basic statistics class at Uni. The problem is that they have simplified what they were taught and incorrectly applied it.
A typical mistake that I have seen is reporting something like “the control group average as 30 and the treated group average was 50 with a less than 5% chance of being random”. Klaxon sounding!!!!
They looked at 100 different bacteria in their study, there is a good chance that 5 of them will have a 5% chance of being significant at random!
Often they will report on averages and appear to assume that the data is a well behaved normal or gaussian distribution.
On occasion, I have looked up the distribution of some of these “discovery” bacteria. The average was not at the 50%ile or median (expected with every normal curve) but at the 87%ile. The mode (most common value) was at the 10%ile.
In short, they are deficient in appropriate skills in handling numbers that arise with the microbiome.
Bottom Line
We need someone to fund serious state-of-the-art research into the microbiome and then evangelize the results into the medical community. This is a hot topic with many many microbiome testing firms being launched by venture capitalists. They see that this has the potential of being financially rewarding.
My own contribution is making a free site that uses data science and artificial intelligence on 16s samples. https://microbiomeprescription.com/ I have seen a few 16s firms, adapt/borrow, features from my site to their clients — I am very fine with that. We are just at the start of the microbiome journey – unfortunately, many still wish that this was just a walk in the park, instead of having to cross the Alps!
I have written almost 1400 blog posts on ME/CFS on this site over the last 9 years (first post was in 2012). One of the first ones was Symptom Mitigation. In recent years, I have focused on the microbiome aspect of ME/CFS – a technical area not suitable for the brain fogged. In this post, I will deal with traditional treatment without using the microbiome, trying to keep things simple for the brain fogged..
Best Feed Back from Readers
Neem has constantly had users surprised, this morning I go this comment on facebook
My post from 2016, Neem – Azadirachta indica gives a summary of the literature at that time. A more recent article is quoted below. There have been no clinical studies on using it with ME/CFS.
Different parts of the plant including flowers, leaves, seeds and bark have been used to treat both acute and chronic human diseases; and used as insecticide; antimicrobial, larvicidal, antimalarial, antibacterial, antiviral, and spermicidal….Over 1000 research articles published on neem has uncovered over 300 structurally diverse constituents, one third of which are limonoids including nimbolide, azadarachtin, and gedunin. These agents manifest their effects by modulating multiple cell signaling pathways.
There are two other Indian Ayurvedic Plants that are well worth trying (one at a time, working from a low dosage up)
Triphala
Tulsi or Holy Basil
My earlier post on Triphala is from 2017, Triphala – an ancient medicine, a more recent post is relevant if your ME/CFS is associated with IBS or leaky gut.
The components of TLP are believed to cause restoration of the epithelium lining of the digestive tract, and by exhibiting mild laxative properties facilitate passage of stool in the colon. TLP is rich in polyphenols, vitamin C and flavonoids, which provide antioxidant and anti-inflammatory effects. It also contains various types of acids, such as gallic, chebulagic and chebulinic, which additionally possess cytoprotective and antifungal properties…Currently, there are no clinical trials assessing the effects of herbal formulations of TLP on clinical course of IBS …
Contrary to pharmaceutical laxatives, which tend to stimulate the bowel, TLP has a regulating effect and can be used long-term. The large intestine is permanently exposed to various toxins, parasites, etc. therefore, it is important to provide adequate bowel cleansing. Literature data indicate that TLP acts as a colon cleanser, which helps to clean the waste matter from the lower GI tract and improve its proper functioning [12, 88]. To sum up, TLP can be particularly helpful if constipation is a symptom, but it can also be useful in some cases of alternating constipation.
A total of 24 studies were identified that reported therapeutic effects on metabolic disorders, cardiovascular disease, immunity, and neurocognition. All studies reported favourable clinical outcomes with no studies reporting any significant adverse events. The reviewed studies reinforce traditional uses and suggest tulsi is an effective treatment for lifestyle-related chronic diseases including diabetes, metabolic syndrome, and psychological stress.
Stress is a Contributor Usually… and we can do something about it
Stress is reported to be a factor in 30-70% of ME/CFS cases. Getting ME/CFS becomes a major source of stress, thus establishing a feedback loop that keeps it going. Stress alter many things in the body. A class of substances classed as adaptogenic, have been found to reduce the alterations in the body. One of these is Tulsi above. There are several others:
“Preparations of Rhodiola rosea root are widely used in traditional medicine. They can increase life span in worms and flies, and have various effects related to nervous system function in different animal species and humans. ” [2020]
“Rhodiola rosea extract is widely used to alleviate stress and improve cognition and mental resources. A total of 50 adult participants were treated with 2 × 200 mg R. rosea extract (Rosalin®, WS® 1,375)…how an improvement of mental speed and moreover, suggest improved mental resources. ” [2020]
“the Rhodiola capsule shows anti-depressive potency in patients with depression disorder when administered in dosages of either 0.3 or 0.6 g/day over a 12-week period.Rhodiola capsule can improve the quality of life and clinical symptoms.The high doses of Rhodiola capsule are better than the lower doses.” [2020]
Most of the above herbs can usually be obtained in bulk as organic powder or as a tea(for example, https://www.starwest-botanicals.com/ ). This means no fillers to react with, nor pesticide residues. Both of these issues have been reported with commercial prepared capsules. It is also cheaper.
The Dilemma of getting a ME/CFS diagnosis
<SOAPBOX> At one time, the official diagnosis criteria was having 4 out of 18 symptoms for no cause being found. Often a diagnosis of IBS or other comorbid diagnosis will be given instead of ME/CFS. Analysis on MicrobiomePrescription.com has found very strong statistical significance of certain symptoms with specific groups of bacteria in the microbiome across many diagnosis. This implies that the symptoms are a reflection of a stable microbiome dysfunction and it’s consequences – imbalances with over 1500 known enzymes, etc. In other words, a complex metabolic disorder.
Readers have often reported that the symptoms disappear when the associated bacteria is normalized. Approaching this issue with a focus on the microbiome is where this blog evolved to.
To translate it from geek speak: what we call ME/CFS is likely several hundred technically different conditions that because of a lack of fine resolution (or any resolution) tests, gets dropped into a large “circular filing cabinet” by most physicians entitle ME/CFS. Unfortunately, because it has a name — it is slotted as a single condition in most medical minds (“It’s a forest with a name” and thus all plants in it are assumed to be the same, thus an Oak and a cloudberry bush are viewed the same). </SOAPBOX>
Please could you write further on Allergic Contact Dermatitis and the microbiome? I am convinced there is a clear connection there, and note one article you reference above specifically supporting the same also. Would be very interested in your holistic take on the same, as you have done with POTS and MCAS.
My approach is always to try to keep to the gold standard, studies on PubMed.
The role of skin and gut microbiome and epigenetic modifications upon skin autoimmune disorders [2020] ” The aim of this review article is to shed new light on some of the commonest skin disorders such as psoriasis, atopic dermatitis, allergic contact dermatitis, with special regards to epigenetic pathogenetic mechanisms such as miRNAs expression and skin and gut microbiome alterations.”
The gut microbiome alterations in allergic and inflammatory skin diseases – an update [2019] “The gut microbiome alterations are linked to the pathogenesis of the allergic, cardiovascular, gastrointestinal, metabolic, neurodevelopmental, psychiatric and neurodegenerative diseases and cancer. Moreover, there is increasing evidence connecting the skin condition with the gastrointestinal microbiome, which has been described as the skin-gut axis.”
Bacterial Dysbiosis and Translocation in Psoriasis Vulgaris [2019] ” Alterations in the gut microbiome have been characterized by a decrease in the Bacteroidetes phylum and an increase in the Faecalibacterium genus… The abundance of Faecalibacterium praunitzii was reduced to a greater extent in patients with both IBD and psoriasis, when compared to patients with only one of the conditions…IBD has been associated with psoriasis since the 1970s (Verbov, 1973; Yates et al., 1982; Lee et al., 1990). However, this association has largely been disregarded. [Also applies to UC and Crohn’s Disease]”
“Constipation was an associated factor for development of atopic dermatitis (AD) (1.17) and AR (1.17), regular intake of lactic acid bacteria was not an associated factor for development of allergic diseases but was a factor for remission of AD (1.22)” [2015]
Bottom Line
At first look, it looks like medical professionals dealing with Allergic Contact Dermatitis and similar conditions, do not want to deal with the gut microbiome. I call this the “It’s not in my wheelhouse” or “I want to keep into my thin silo” syndrome. There is a nasty situation created by excessive specialization of medicine and medical research.
I hate to say it, but the fastest way forward (and to get relief) may be doing citizen science via https://microbiomeprescription.com/ This depends on people with Allergic Contact Dermatitis getting appropriate 16s tests (see suitable providers here as well as which ones are most popular here). The site will automatically show relationships once we get 20 or more annotated samples uploaded.
I have added these to the symptom list on the site.
In writing another post, I discovered that I had not included this in my review of adaptogenic supplements. Adaptogenic means something that moderates the impact of stress. Stress is very common with ME/CFS and should not be ignored. The earlier posts were:
“These findings suggest that ashwagandha’s stress-relieving effects may occur via its moderating effect on the hypothalamus-pituitary-adrenal axis.” [2019]
“The treatment group that was given the high-concentration full-spectrum Ashwagandha root extract exhibited a significant reduction (P<0.0001) in scores on all the stress-assessment scales on Day 60, relative to the placebo group. ” [2012]