Many support groups provide lists of local MDs that are sympathetic to ME/CFS patients. Typically, they will attempt to do symptom relief, not remediate the underlying cause or do not test outside of their local standards of practice (i.e. testing for associated viral infection, Lyme or rickettsia infections) – independent of insurance coverage or the patient being will to pay.
The family was extremely fortunate to be covered by the old Microsoft Medical insurance that covered everything that the MD wanted with no deductibles; and we had a MD that was willing to learn and explore.
The Clinical and Scientific Basis of Myalgic Encephalomyelitis – Edited by Byron Hyde, M.D. Free Download eBook (PDF) This is a collection of a massive number of early research papers — most still relevant.
Goodreads: Me Cfs Books, I would exclude books not written by a MD or published before 2020.
Note that the better books are often difficult or impossible to understand due to brain fog (and sometime lack of sufficient education is specific areas)
Determine a Model and if possible, see if there is evidence that the model works
I went with two models for ME/CFS: A hypercoagulation condition (David Berg) and an “occult rickettsia like infection” (Cecile Jadin); today we could call it “post Infection Fatigue Syndrome”. Both were testable (by lab or by reaction to low risk drugs, i.e. an antibiotic often prescribed for Acne) and actionable.
Today, my thinking is that the simplest model is a persistent microbiome dysfunction. This is very testable with direct retail tests; and actionable (using Microbiome Prescription). Often the antibiotics suggestions from Microbiome Prescription mirrors the Jadin approach. The treatment plan works for her models and my microbiome model!
Going with a hypothesis that is not both testable and actionable is not recommended. Take action today incase it works! Leave speculations to researchers trying to get grant money for their special interests.
Symptoms and Bacteria appears to be strongly related
It is typical that Microbiome Prediction correctly predicts 80-100% of a person’s dominant symptoms from their microbiome. This implies that the bacteria shifts are causing the symptoms; thus correcting the bacteria shifts may reduce or eliminate symptoms.
“Methylomes of the blood cells of patients with FM and CFS in three independent studies have shown methylation changes that appear to be implicated in the pathogenesis of these syndromes.”
Well known, see MEPedia, treatment based on this hypothesis has not been effective for most
” both long COVID and ME/CFS patients exhibit similarly impaired endothelial function, indicating potential vascular involvement in the pathogenesis of these post-viral illnesses. The significant reduction in flow-mediated dilation values suggests an increased cardiovascular risk”
“Biomarkers of intestinal barrier function and inflammation were associated with autonomic dysfunction assessed by COMPASS-31 scores in FM and ME/CFS respectively. Anti-β-LGB antibodies, ZO-1, LPS, and sCD14 may be putative predictors of intestinal barrier dysfunction in these cohorts.”
Well known from prior studies, causality not explored.
“Regional alterations were most frequently identified in the cerebral cortex, with a notable focus on the frontal cortex. However, our meta-analysis data revealed a significant hypoactivity in the insular and thalamic regions, contrary to observed frequencies. These abnormalities, occurring in pivotal network hubs bridging reason and emotion, disrupt connections with the limbic system, contributing to the hallmark symptoms of ME/CFS.”
“In patients with CFS, TCME probably reduces post-intervention fatigue, depression, and anxiety and may improve sleep quality and mental function compared with passive control, but has limited long-term effects. “
“The prospective research directions in this field include the search for biological markers, with a particular focus on immunology; the advancement of diagnostic techniques; the screening of risk genes associated with CFS; and the conduct of epidemiological investigations.”
So treatment does not seem to be an active dimension.
“recommendations of T&CMs in treating CFS remain inconclusive. To develop better quality evidence about T&CMs for CFS, future studies should employ more objective diagnosis standards and outcome measurements, larger sample size, and better bias control, and ensure the compliance with the corresponding reporting guidelines”
I have seen this constantly in studies: too small sample size, poor statistical analysis, spinning results to “find something”.
“In conclusion, since this was a case study based on self-assessments by a small number of patients and not a clinical study”
Hydrogen is a gas used by bacteria (illustrated by SIBO testing for Hydrogen), this approach is likely to influence the microbiome. Looking at the data on Microbiome Prescription, we found that ME/CFS patients microbiome has a significantly higher consumption of Hydrogen — thus the extra hydrogen may alter the microbiome.
Glucan (or foods containing it: Barley etc) is a very frequent suggestion from Microbiome Prescription when a ME/CFS microbiome was processed through microbiome prescription.
Some symptoms improved: “orthostatic intolerance with the inability to complete the 10-min standing test was resolved in 10 (83%) out of 12 patients, and disequilibrium was resolved in 15 (88%) out of 17 patients. “
Beta-Glucan (or foods containing it: Barley etc) is a very frequent suggestion from Microbiome Prescription when a ME/CFS microbiome was processed through microbiome prescription.
“significantly improved cognitive fatigue (assessed with FIS-40 scores) after the 36-week treatment
The earliest use of antibiotics for treating ME/CFS that I am aware of, dates from the late 1990’s with articles in Journal of Chronic Fatigue Syndrome (and conference reports prior)
My remission from ME/CFS was done by combining C.L. Jadin protocol with Dave Berg anticoagulant protocol.
Overview of results
First, let us show the numbers and then talk about them. It is clear that there are significant changes. There are a lot of dimensions to consider.
Criteria
2-Mar
9-Mar
21-Mar
3-Apr
16-Jun
Shannon Diversity Index (Percentile)
85.2
79.0
99.8
72.4
16.0
Simpson Diversity Index (Percentile)
72.6
63.4
64.4
77.0
91.4
Chao1 Index (Percentile)
65.7
31.2
77.2
62.9
7.9
Lab Read Quality
8.9
8.7
6
4.5
4.4
Bacteria Reported By Lab
654
533
725
585
389
Bacteria Over 99%ile
2
4
30
11
24
Bacteria Over 95%ile
13
10
70
33
38
Bacteria Over 90%ile
25
23
103
63
55
Bacteria Under 10%ile
287
213
123
113
140
Bacteria Under 5%ile
253
173
66
48
96
Bacteria Under 1%ile
219
135
17
8
46
Lab: BiomeSight
Rarely Seen 1%
13
1
38
5
6
Rarely Seen 5%
28
9
107
17
29
Pathogens
36
31
50
40
36
Outside Range from JasonH
6
6
9
9
8
Outside Range from Medivere
15
15
22
22
22
Outside Range from Metagenomics
7
7
9
9
9
Outside Range from MyBioma
5
5
6
6
6
Outside Range from Nirvana/CosmosId
26
26
18
18
15
Outside Range from XenoGene
28
28
46
46
42
Outside Lab Range (+/- 1.96SD)
6
8
56
17
27
Outside Box-Plot-Whiskers
44
36
124
70
67
Outside Kaltoft-Moldrup
233
169
207
137
170
Condition Est. Over 99%ile
0
0
13
10
48
Condition Est. Over 95%ile
1
0
24
35
75
Condition Est. Over 90%ile
2
2
34
55
84
Enzymes Over 99%ile
0
0
347
606
957
Enzymes Over 95%ile
7
0
635
970
1145
Enzymes Over 90%ile
24
28
746
1159
1228
Enzymes Under 10%ile
506
515
561
237
245
Enzymes Under 5%ile
378
360
422
143
174
Enzymes Under 1%ile
194
166
120
52
94
Compounds Over 99%ile
0
0
225
215
617
Compounds Over 95%ile
2
0
355
410
732
Compounds Over 90%ile
8
11
441
520
778
Compounds Under 10%ile
1243
986
1105
902
822
Compounds Under 5%ile
1156
926
1032
856
796
Compounds Under 1%ile
1115
875
936
828
767
Next are the percentages by percentile which I noticed tend to have over representation with ME/CFS and Long COVID in the 0-9 percentile. We see this pattern at the start, with improvement and then a bounce back to high numbers.
2-Mar
2-Mar
9-Mar
9-Mar
21-Mar
21-Mar
3-Apr
3-Apr
16-Jun
16-Jun
Percentile
Genus
%
Genus
%
Genus
%
Genus
%
Genus
%
0 – 9
65
40%
51
36%
28
15%
29
19%
35
36%
10-19
13
8%
16
11%
36
19%
23
15%
9
9%
20 – 29
11
7%
16
11%
20
11%
23
15%
14
14%
30 – 39
5
3%
9
6%
17
9%
17
11%
4
4%
40 – 49
13
8%
10
7%
14
8%
11
7%
5
5%
50 – 59
12
7%
8
6%
10
5%
8
5%
3
3%
60 – 69
12
7%
9
6%
6
3%
14
9%
1
1%
70 – 79
12
7%
3
2%
10
5%
6
4%
5
5%
80 – 89
10
6%
10
7%
15
8%
9
6%
7
7%
90 – 99
11
7%
8
6%
30
16%
15
10%
15
15%
Total
164
140
186
155
98
2-Mar
2-Mar
9-Mar
9-Mar
21-Mar
21-Mar
3-Apr
3-Apr
16-Jun
16-Jun
Percentile
%
Species
%
Species
%
Species
%
Species
%
Species
0 – 9
41%
94
43%
79
13%
40
17%
36
21%
31
10-19
6%
14
9%
16
15%
44
13%
28
9%
13
20 – 29
8%
18
9%
16
13%
39
12%
27
15%
22
30 – 39
3%
7
5%
10
10%
29
10%
22
8%
11
40 – 49
7%
17
4%
7
7%
20
8%
17
6%
9
50 – 59
9%
21
5%
9
7%
22
6%
12
5%
7
60 – 69
6%
14
8%
14
3%
10
6%
14
6%
9
70 – 79
8%
18
4%
7
6%
19
7%
15
6%
9
80 – 89
6%
13
8%
15
8%
23
8%
17
10%
14
90 – 99
5%
12
6%
11
19%
57
13%
29
14%
21
Total
228
184
303
217
146
The Events Around the above Samples
2023-03-02 (baseline)
2023-03-09 (during a stomach bug)
2023-03-21 (during a “Level 1” remission while taking Amoxiclav. Level 1 = all symptoms gone. Felt great. Had started Amoxiclav on the morning of 3/20, this sample was taken after 3 doses around 3pm)
2023-04-03 (4 days after stopping Amoxiclav, was on Doxycycline)
2023-06-16 (During 2nd round of Amoxiclav when I felt really bad)
The microbiome results definitely reflected the Level 1 remission on 3-21. The low percentile genus and species percentage almost made it to the target level of 10% from the prior 40%! The Shannon Diversity Index was awesome (the higher the better!).
I have often described correcting the microbiome as being similar to sailing a sailboat along a coast line. Depending on wind and tide, there may be a lot of course changes required. I am curious on the ranking of Amoxiclav[amoxicillin] and Doxycycline with these samples. The numbers below suggests that going on to Doxycycline may have been a poor choice. On the 2nd round of Amoxiclav, it was at just 35% of the highest value recommendation versus 70% on the 1st round.
Note that rifaximin and rifampicin are in the same family and used by some ME/CFS specialists. Imipenem shows up often with ME/CFS samples — but since it is intravenous, not the easiest to get on an ongoing basis.
Take Away and Reflections
This project main purpose was to show that remission can be triggered by antibiotics to another generation of people suffering from ME/CFS. The remission on 21-Mar demonstrates this to be correct both subjectively and objectively (Microbiome data — specifically Shannon Diversity Index and Percentages in different percentiles for Species and Genus). I should emphasis that both of these measures are multi-bacteria measures and do not support the common myth that ME/CFS is caused by a single bacteria.
The critical issue is maintaining remission. How do keep the microbiome where it should be. I often use analogies of cities because we are talking about a city of bacteria. To stop riots and looting in the streets you send in the National Guard (antibiotic). The city is back to normal. The causes of the the riots are still there. Typically lack of opportunities, neglect, etc. in these same ghettos. You must address these other issues. A repeat of sending in the National Guard may have the same effect as the first time OR very different effects – the same can be said for using the same antibiotics.
With bacteria we have two “radical organizations in the ghetto” — The Antibiotic resistant and the Resistors. For example, the bacteria that survive learnt how to avoid the National Guard and proceed to share that skill to other bacteria. Instead of a wall of shields pushing the rioters back, Molotov cocktails rain down on the troops from above.
Another analogy is that the gut is a pendulum. The antibiotics, probiotics and other items pushes the gut towards the equilibrium position! There is great joy! The gut is centered… At this point, many people go down the wrong reasoning path — “Keep doing more of the same to stay in remission!“. Remission is lost and the momentum pushes the guts out to the other side!!! You pushed out one devil and seven more devils return! (Math 12:43-45)
The key is to dampen down the swing so there is less and less swing. My personal opinion is that Cecile Jadin’s protocol using antibiotics for only 7 days each month is a very effective way of dampening the pendulum gained from decades of experience.
My approach with Microbiome Prescription is to try to address the whole city. Before taking action, we get intelligence on the nature of the city and decide on the appropriate action for a period of time (typically 4-10 weeks). We then update our intelligence (i.e. microbiome test) and pick the next course of action. Actions may include “food kitchens”, “safe injection sites”, “training programs”, “home repairs”, “on the beat policing”, etc.
There are many people who will state that antibiotics gave me ME/CFS. I do not disagree. Antibiotics can also trigger remission — the problem is WHICH antibiotics. Since every person’s microbiome is unique, there can be no universal “best antibiotic” for ME/CFS. Antibiotics must be selected based on the individuals microbiome (which is the path that Microbiome Prescription took) for the best odds of making the right choice.
My Suggestions Going Forward
I am working with C.L. Jadin, M.D., on documenting her current protocol from almost 30 years of experience using antibiotics for ME/CFS. It will be out soon. I am hoping to have that available within a month. One key aspect of her protocol has been pulsing antibiotics using two at a time. There are a few studies showing that pulsing is more effective. Pulsing often means 7 days on and 21 days off.
Looking at Tess’s last sample, I would propose the following to be considered (items that I picked from the consensus suggestions):
Take a 3 week break from antibiotics (Ideally at the end take another sample)
A common pattern of people is “Just give me a pill to fix me, I want to keep my current life style and I am not prepared to make significant life style and diet changes”. My impression is that making those changes is often required. Inertia is a real maintainer of ME/CFS, especially the pendulum inertia when trying to heal.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide information on rotations etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.
For more information on this project see Health Rising post. Both participants has granted me to do a review with their real names. This is the second of a series of posts on this project, the first one was on The Remission Biome Project: Tess Falor.
The earliest use of antibiotics for treating ME/CFS that I am aware of, dates from the late 1990’s with articles in Journal of Chronic Fatigue Syndrome (and conference reports prior)
My remission from ME/CFS was done by combining C.L. Jadin protocol with Dave Berg anticoagulant protocol.
A big thanks to BiomeSight.com for donating some testing kits to the project. If interested in using their kits, there is a discount code (“micro”).
Overview of results
First, let us show the numbers and then talk about them. It is clear that there are significant changes. There are a lot of dimensions to consider. Some highlights:
The number of bacteria with abnormally high representation has gone from 123 down to 29
The number of bacteria with abnormally low representation has gone from 222, dropping down to as low as 19, before rebounding to 162 (still better than the start)
Most measure showed great improvement and then some relapse.
Criteria
7-Mar
23-Mar
15-Apr
22-Apr
29-Apr
Shannon Diversity Index
33.8
78.0
97.1
76.5
77.1
Simpson Diversity Index
0.7
65.1
58.6
60.3
73.4
Chao1 Index
91.3
61.6
72.0
89.4
14.8
Chi-Square (Lower is better)
55
47
46
50
30
Lab Read Quality
8.6
7.1
5.4
2.2
6.9
Bacteria Reported By Lab
755
638
628
765
461
Bacteria Over 99%ile
27
11
13
56
5
Bacteria Over 95%ile
72
25
30
105
18
Bacteria Over 90%ile
132
46
63
178
29
Bacteria Under 10%ile
222
218
62
19
162
Bacteria Under 5%ile
191
195
18
12
144
Bacteria Under 1%ile
177
179
0
3
112
Lab: BiomeSight
Rarely Seen 1%
8
4
3
66
2
Rarely Seen 5%
22
24
27
128
14
Pathogens
39
32
33
31
29
Outside Range from JasonH
8
8
8
8
8
Outside Range from Medivere
18
18
16
16
16
Outside Range from Metagenomics
9
9
6
6
6
Outside Range from MyBioma
10
10
6
6
6
Outside Range from Nirvana/CosmosId
18
18
12
12
12
Outside Range from XenoGene
52
52
39
39
39
Outside Lab Range (+/- 1.96SD)
43
15
17
36
7
Outside Box-Plot-Whiskers
146
51
83
227
43
Outside Kaltoft-Moldrup
251
189
105
212
158
Condition Est. Over 99%ile
1
5
0
0
3
Condition Est. Over 95%ile
2
14
0
5
13
Condition Est. Over 90%ile
11
28
2
11
21
Enzymes Over 99%ile
7
68
5
19
37
Enzymes Over 95%ile
22
281
209
123
250
Enzymes Over 90%ile
58
435
361
317
409
Enzymes Under 10%ile
219
354
59
48
201
Enzymes Under 5%ile
173
265
34
24
144
Enzymes Under 1%ile
138
94
13
12
79
Compounds Over 99%ile
3
44
1
13
16
Compounds Over 95%ile
15
186
82
68
87
Compounds Over 90%ile
27
297
154
153
183
Compounds Under 10%ile
882
889
985
987
875
Compounds Under 5%ile
862
859
959
963
841
Compounds Under 1%ile
845
802
935
952
820
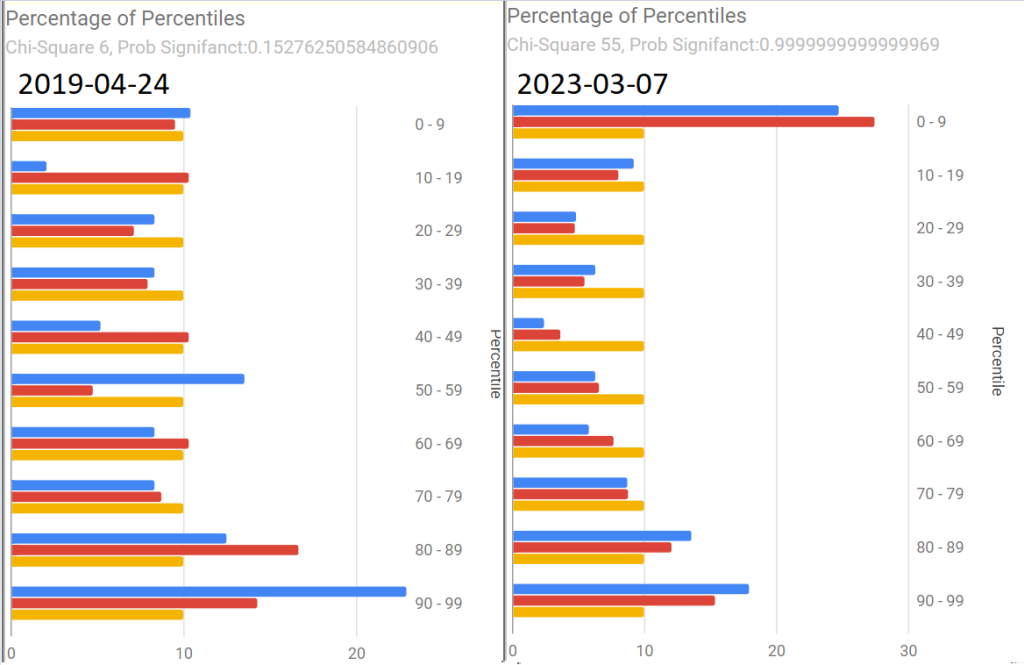
As with Tess, the percentages by percentile which I noticed tend to have over representation with ME/CFS and Long COVID in the 0-9 percentile. We see this pattern at the start, with improvement and then a bounce back to high numbers in the last sample
Tamara suggested that I convert the tables below to charts. Both are now available on the site.
Pretty Pictures
Tamara suggested that I convert the tables below to charts. Both are now available on the site.
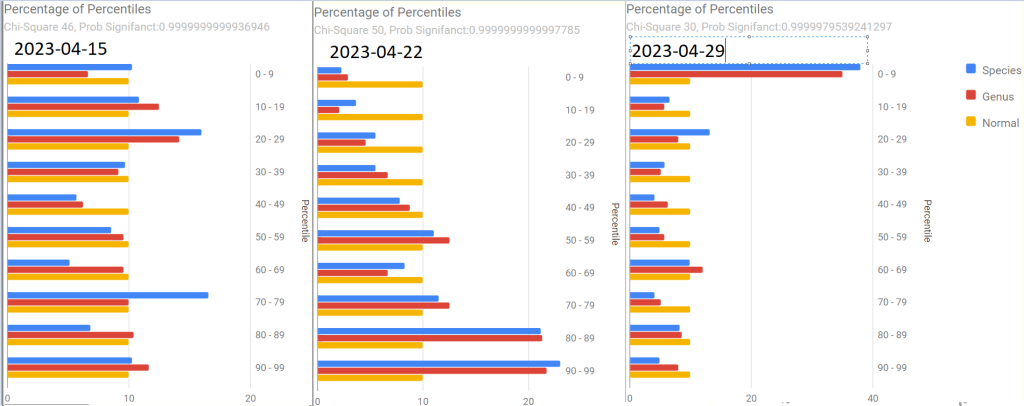
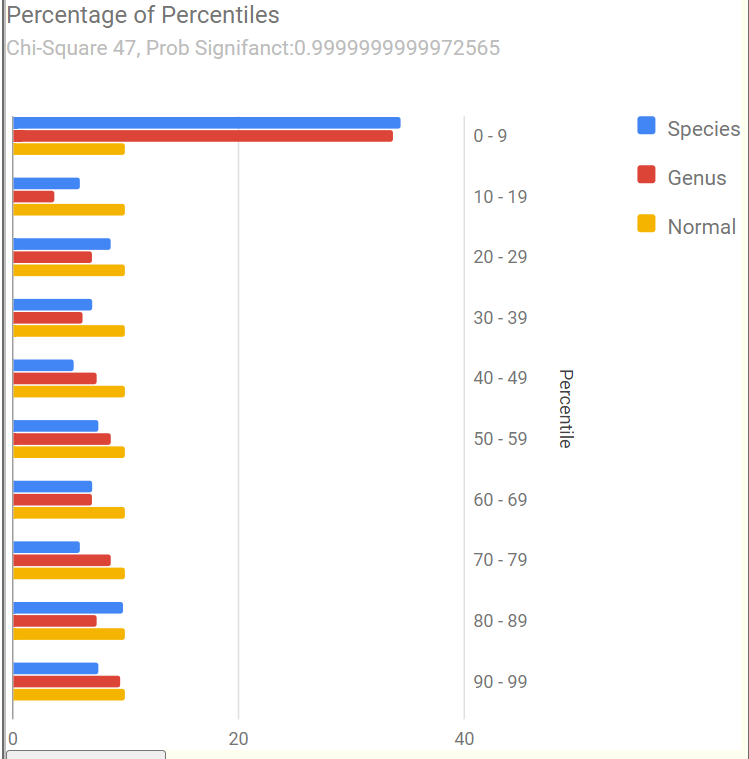
First, an old sample that she happened to have where we see Chi-Square at 6. The first of the recent samples had it jumping to 55, A normal microbiome is expected to have a Chi-square < 13. A higher value indicates a statistically significant, abnormal microbiome.
The next three show the changes with antibiotics. Chi-square went from 46 to 50 with a dramatic shift and then drifted down to 30.
The latest sample increased upward again, with the pronounced spikes that are common with ME/CFS being there.
The raw numbers are also shown. I will spare your eyes by omitting them.
The Events Around the above Samples
7 Mar – Before
23 Mar – Day 4 AmoxClav
15 Apr – More
22 Apr – Final Day of AmoxClav (30 days of AC)
This sample has a low Lab Read Quality, this may account for the number of spikes in its report.
29 April – After 3 days of Aprepitant + Erythromycin (this was a BIG difference from Tess and was the intervention that seemed to give me the baseline increase this time).
As with Tess, let us see how these items rank in each sample. As with Tess, imipenem is the most common best suggestion.
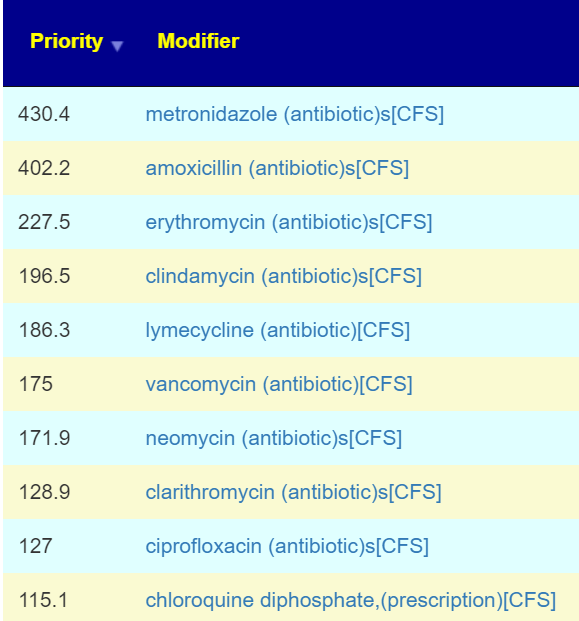
As a result of a conference call with some of the Remission Biome Project, and Dr. Jadin’s Current Protocol for ME/CFS. I annotated all of the antibiotics used in studies for ME/CFS, Lyme, and related conditions with [CFS]. This allows us to quickly see the “consensus” antibiotics (i.e. used in studies and suggested by microbiome prescription algorithms).
The top ones are shown before (Just enter “CFS” in the Search dialog)
Only two of these were negative for her (doxycycline and ampicillin) with docycline sibling, minocycline being just 21).
I would suggest using this list to pick 2 antibiotics to do a one week course and then take a 3 week break. After the course, then do some of these probiotics. I am inclined to omit L.Casei because the strain used in Yakult is a negative. Thus we end up with these three as top suggestions. P.S.
Note the weight of these are above many of the antibiotics above. I usually advocate single species. The Bifido is available from Custom Probiotics with their recommended dosages above the amount listed above.
Part Deux — More Samples!
Her description of subjective changes: generally keep improving in terms of PEM, function etc. (was definitely a dip around the 2nd ‘constipation’ sample)
1st, [2023-06-14] in the series just a temporal sample, no additional treatments
2nd, [2023-07-15] in the series I had a major episode of constipation – wanted to catch that
3rd, [2023-07-20]last one was was post my 2nd treatment of aprepitant+erythromycin
Sample Comparison
We include the prior one above for easy reference). The key change items are:
The new Anti inflammatory Bacteria Score has seen a dramatic increase from 17%ile to 73%ile. The four prior samples were 7.6%ile, 8.2%ile, 3.9%ile and 6.9%ile
Outside Kaltoft-Moldrup is dropping. In terms of %age of reported: 32% -> 28% -> 29% ->16%
The high and low Enzymes also seem to be dropping
The last sample had a Chi-Square of 9, that is a probability of 0.54 instead of the .9999999… for all other samples. Unfortunately, the poor read quality makes this fuzzy.
Note: The last sample has a low read quality (thus less bacteria types are being reported)
Criteria
22-May
14-Jun
15-Jul
22-Jul
Shannon Diversity Index
69.4
29.20
43.00
15.00
Simpson Diversity Index
54.7
7.60
27.50
60.00
Chao1 Index
72.4
0.87
21.40
8.30
Anti inflammatory Bacteria Score
17.0
30.90
43.60
73.20
Chi-Square Score
49
51
32
9
Lab Read Quality
7.2
10.9
6.6
2.3
Bacteria Reported By Lab
659
752
512
375
Bacteria Over 99%ile
10
12
1
4
Bacteria Over 95%ile
22
24
2
20
Bacteria Over 90%ile
45
41
13
39
Bacteria Under 10%ile
199
229
189
19
Bacteria Under 5%ile
186
208
184
3
Bacteria Under 1%ile
167
165
166
0
Lab: BiomeSight
Rarely Seen 1%
25
13
0
0
Rarely Seen 5%
49
37
7
1
Pathogens
32
34
36
21
Outside Range from JasonH
4
7
7
4
Outside Range from Medivere
14
19
19
14
Outside Range from Metagenomics
6
7
7
6
Outside Range from MyBioma
4
6
6
4
Outside Range from Nirvana/CosmosId
18
19
19
18
Outside Range from XenoGene
33
34
34
33
Outside Lab Range (+/- 1.96SD)
11
12
1
13
Outside Box-Plot-Whiskers
56
75
23
50
Outside Kaltoft-Moldrup
209
212
150
61
Condition Est. Over 99%ile
0
0
1
0
Condition Est. Over 95%ile
0
0
1
0
Condition Est. Over 90%ile
1
0
3
0
Enzymes Over 99%ile
62
1
5
2
Enzymes Over 95%ile
130
3
18
11
Enzymes Over 90%ile
215
12
99
33
Enzymes Under 10%ile
429
211
171
304
Enzymes Under 5%ile
310
146
142
211
Enzymes Under 1%ile
152
85
73
47
Compounds Over 99%ile
31
0
3
1
Compounds Over 95%ile
64
2
9
11
Compounds Over 90%ile
106
7
48
24
Compounds Under 10%ile
959
1096
1009
1015
Compounds Under 5%ile
909
1041
981
971
Compounds Under 1%ile
860
1009
956
922
Since we had a symptom of constipation, let us see how well the samples match that reported from Studies on PubMed — there were no matched. When we went to our Special Studies, we see that the microbiome followed the reported symptoms. We then look at the top value from Special Studies — which was Long COVID for all samples. We see the lost of ground around the constipation and then regaining the progress.
Criteria
22-May
14-Jun
15-Jul
22-Jul
Special Studies
7%ile
14%ile
15%ile
7%ile
Top Item Long COVID
35 %
44 %
41 %
36 %
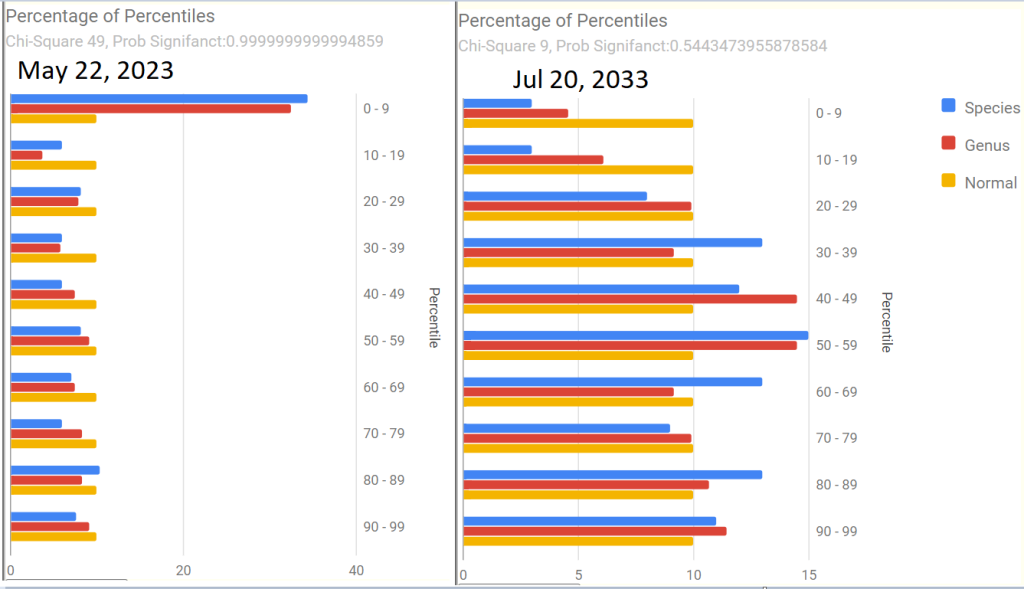
Next we go and look at aprepitant and erythromycin
The Percentage of Percentile show quite a shift — unfortunately, it is unclear if this is a temporary after effect of constipation, poor lab read quality, or the above aprepitant and erythromycin. The next sample may resolve this issue.
Is the Project working — YES
We are seeing both subjective improvement and object improvements.
Personally, I like what appears to be a shift towards Cecile Jadin’s approach — not continuous antibiotics but a course (7-10 days) followed by a break (ideally 3 weeks). Often I find that ME/CFS people tend to be impatient and just want to keep pressing on hard… which I have observed often result in tripping and rolling down the hill to where they were (or worst).
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide information on rotations etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.