
Brain Scans
Brain “fog” and cognitive issues have often resulted in brain scans being done of CFS patients. A brain scan does not usually help with treatment; it simply suggests why some symptoms occur. The typical report conclusion is hypoperfusion, meaning too little blood getting to the brain tissue. CFS patients have frequently had several types of brain scans with modern technology. The main methods are:
- Magnetic Resonance Imaging (MRI)
- Positron Emission Tomography (PET)
- Transcranial Doppler Sonography (TDS)
- Single-photon emission computerized tomography (SPECT)
SPECT scans have been the most consistent for finding issues with the CFS patients, with 80% finding distinct abnormal results.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) studies are hit-and-miss for showing abnormalities. Approximately 27% – 32% of CFS patients show abnormal scans. Approximately 14% of chronic Lyme patients show abnormal scans. MRIs are often normal and of limited usefulness (except to exclude other conditions). MRIs are affected by Jarisch-Herxheimer Reactions (JHR); this implies MRI results will change as symptoms wax and wane. Similarly, if the patient has done fatiguing tasks recently, the MRI results may change.
MRI scans are useful; one study found that 35% of abnormal scans (10% of CFS patients scanned) suggest other known medical causes. CFS subjects with MRI brain abnormalities report being more physically impaired than those patients without brain abnormalities. MRIs are useful for excluding other possible causes for the fatigue.
MRI studies found varying issues (i.e. lack of consistency) for CFS patients.
- Abnormalities seen in 78% of EBV-associated CFS patients
- Abnormalities in 14% of chronic Lyme patients
- Decrease in grey matter volume, 1% decrease per year with CFS. (2011)
- Decrease in white matter volume with level of fatigue, also seen with chronic Lyme
- Greater effort—exertion—to process auditory information
- Greater activity in several cortical and subcortical regions during the fatiguing cognitive task
- Increased activation in the occipito-parietal cortex, posterior cingulate gyrus and parahippocampal gyrus, and decreased activation in dorsolateral and dorsomedial prefrontal cortice
- MRI abnormalities consisted of foci of T2-bright signal in the periventricular and subcortical white matter and in the centrum semiovale
- No abnormal patterns in rate and extent of brain atrophy, ventricle volume, white matter lesions, cerebral blood flow or aqueduct CSF flow
- Significant differences in brain activation between two groups as the demands of the task increased
- “CFS, as diagnosed by Centers for Disease Control and Prevention criteria, is not a clinical entity reliably associated with reduced GMV [using MRI] “. [2017]
- “We found a significant decrease in WM volumes in the left inferior fronto-occipital fasciculus (IFOF) in CFS while in normal controls it was unchanged [comparing MRI results taken 6 years apart” [2016]
- “Abnormal regressions were detected in nuclei of the brainstem vasomotor centre, midbrain reticular formation and hypothalamus, but also in limbic nuclei involved in stress responses and in prefrontal white matter [of individual patients]. Group comparisons of CFS and NC did not find MRI differences in these locations” [2016]
- “changes of uncertain significance were identified by MRI and lumbar puncture in a few patients.” [2016]
- Other studies found changes in state when MRI was done doing challenges etc. i.e. speed of response was different from normal controls
As an unexpected fact, Crohn’s disease also shows MRI variations. Results for irritable bowel syndrome are mixed.
References:
- http://www.ncbi.nlm.nih.gov/pubmed/20223910 (2010)
- http://www.ncbi.nlm.nih.gov/pubmed/9282853 (1997)
- http://www.ncbi.nlm.nih.gov/pubmed/10761837 (2000)
- http://www.ncbi.nlm.nih.gov/pubmed/8138812 (1993)
- http://www.ncbi.nlm.nih.gov/pubmed/9282853 (1997)
- http://www.ncbi.nlm.nih.gov/pubmed/21042805 (2011)
- http://www.ncbi.nlm.nih.gov/pubmed/18302644 (2008)
- http://www.ncbi.nlm.nih.gov/pubmed/8138812 (1993)
- http://www.ncbi.nlm.nih.gov/pubmed/11328679 (2001)
- http://www.ncbi.nlm.nih.gov/pubmed/21560176 (2011)
- http://www.ncbi.nlm.nih.gov/pubmed/15955487 (2005)
- P.7 http://www.investinme.org/Documents/MECFS%20Conference%202012/Ros%20Vallings%20IIMEC7%20Report.pdf
- http://www.ncbi.nlm.nih.gov/pubmed/20223910 (2010)
- http://www.ncbi.nlm.nih.gov/pubmed/8141020 (1994 )
- http://www.ncbi.nlm.nih.gov/pubmed/18447963 (2008)
- http://www.ncbi.nlm.nih.gov/pubmed/17408973 (2007)
- http://www.ncbi.nlm.nih.gov/pubmed/17079703 (2006)
- http://www.ncbi.nlm.nih.gov/pubmed/15907308 (2005)
- http://www.ncbi.nlm.nih.gov/pubmed/1309285 (1992)
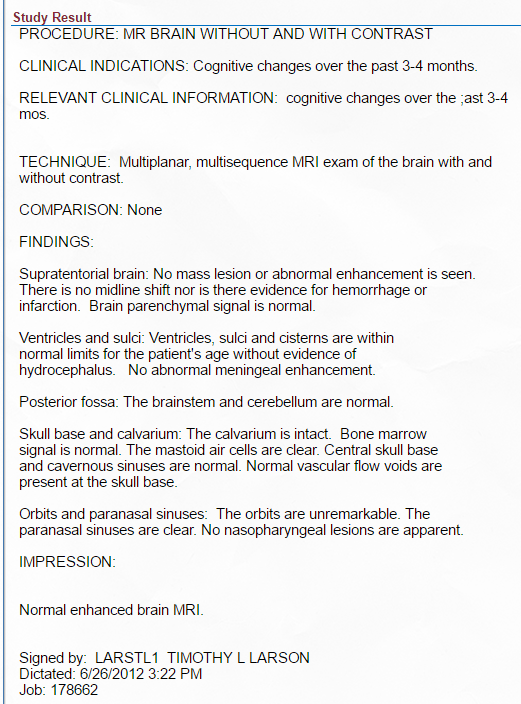
Example of one CFS patient — below is same patient with a SPECT scan
Positron emission tomography
- 50% of CFS patients show abnormal scans
- Significant hypometabolism in right mediofrontal cortex and brainstem
- Hypometabolism bilaterally in the cingulate gyrus and the adjacent mesial cortical areas, decreased metabolism in the orbitofrontal cortex
- Decreased 5-HT1A receptor number affinity
- Neuroinflammation in Patients with Chronic Fatigue Syndrome/Myalgic Encephalomyelitis: An 11C-(R)-PK11195 PET Study.[2014]
Reference
- http://www.ncbi.nlm.nih.gov/pubmed/12810781 (2003)
- http://www.ncbi.nlm.nih.gov/pubmed/9790483 (1998)
- http://www.ncbi.nlm.nih.gov/pubmed/12810781 (2003)
- http://www.ncbi.nlm.nih.gov/pubmed/15691524 (2005)
Transcranial Doppler Sonography
- Cerebral blood flow is less effective with POTS (slower response)
- Less cerebral blood flow in patients with CFS than controls
- Shorter time to orthostatic symptoms in patients with CFS
Reference
- http://www.ncbi.nlm.nih.gov/pubmed/19502561 (2009)
- http://www.ncbi.nlm.nih.gov/pubmed/22180650 (2012)
- http://www.ncbi.nlm.nih.gov/pubmed/12593133 (2003)
SPECT
Single-photon emission computerized tomography (SPECT) scans are the most reliable for CFS.
- 80% of CFS patients show abnormal scans
- 70% of chronic Lyme patients have abnormal scans
- Abnormalities in perfusion to the frontal, temporal, and parietal lobes
- SPECT abnormalities appeared to correlate with clinical status
- Defects were located predominantly in the frontal and temporal lobes. Midcerebral uptake index was found to be significantly lower
- Lower cortical/cerebellar rCBF ratios in CFS patients
- In monozygotic twins (one with CFS, one without CFS), the same patterns were seen
- 80% of CFS patients had lower than average global cerebral blood flow
- CFS patients had diffuse regional cerebral blood flow
- Abnormal cerebral perfusion patterns in CFS patients
- CFS patients had reduced absolute cortical blood flow in rather broad areas
- CFS patients had reduced cortical blood flow in the distribution of both right and left middle cerebral arteries
- Blood flow in the left basal ganglia and thalamus was markedly higher in CFS patients
- Serum TGF-beta and cerebral blood flow abnormalities were accentuated after exercise in CFS patients
Similar results were seen with Chronic Lyme Disease.
Reference
- http://www.ncbi.nlm.nih.gov/pubmed/8141020 (1994)
- http://www.ncbi.nlm.nih.gov/pubmed/18447963 (2008)
- http://www.ncbi.nlm.nih.gov/pubmed/17408973 (2007)
- http://www.ncbi.nlm.nih.gov/pubmed/17079703 (2006)
- http://www.ncbi.nlm.nih.gov/pubmed/15907308 (2005)
- http://www.ncbi.nlm.nih.gov/pubmed/1309285 (1992)
- http://www.ncbi.nlm.nih.gov/pubmed/12810781 (2003)
- http://www.ncbi.nlm.nih.gov/pubmed/9790483 (1998)
- http://www.ncbi.nlm.nih.gov/pubmed/12810781 (2003)
- http://www.ncbi.nlm.nih.gov/pubmed/15691524 (2005)
- http://www.ncbi.nlm.nih.gov/pubmed/19502561 (2009)
- http://www.ncbi.nlm.nih.gov/pubmed/22180650 (2012)
- http://www.ncbi.nlm.nih.gov/pubmed/12593133 (2003)
- http://informahealthcare.com/doi/abs/10.1300/J092v03n01_05 (1997)
- http://www.ncbi.nlm.nih.gov/pubmed/1491843 (1992)
- http://www.ncbi.nlm.nih.gov/pubmed/8141020 (1994)
- http://www.ncbi.nlm.nih.gov/pubmed/8141020 (1994)
- http://www.ncbi.nlm.nih.gov/pubmed/8141022 (1994)
- http://www.ncbi.nlm.nih.gov/pubmed/1491843 (1992)
- http://www.ncbi.nlm.nih.gov/pubmed/11376266 (2001)
- http://www.ncbi.nlm.nih.gov/pubmed/21167506 (2011)
- http://www.ncbi.nlm.nih.gov/pubmed/12554824 (2003)
- http://www.ncbi.nlm.nih.gov/pubmed/10974961 (2000)
- http://www.ncbi.nlm.nih.gov/pubmed/8542261 (1995)
- http://www.ncbi.nlm.nih.gov/pubmed/16494597 (2006)
- http://www.ncbi.nlm.nih.gov/pubmed/16494597 (2006)
- http://www.ncbi.nlm.nih.gov/pubmed/10761837 (2000)
- http://www.ncbi.nlm.nih.gov/pubmed/7496949 (1994)
- http://www.ahmf.org/01access/01casse.html (2001)
- http://www.cfs-news.org/aacfs-01.htm (2001)
Below is the SPECT scan of the CFS person that had a normal MRI

My own experience
Family member had > 60% abnormalities with SPECT (done by Dr. Daniel Amen himself). My MRI was completely normal, my SPECT was not.
IMHO: Obtaining a SPECT scan is one of the best diagnostic tests for CFS for two reasons:
- 80% chance of getting a positive result if you have CFS
- It shows that the issue is a physical neurological issue and not a psychological issue.
Do not get talked into a MRI with claims that it is “equivalent or better”.
NEW STUDY: SPECT IS BEST FOR BRAIN INJURY DIAGNOSIS AND TREATMENT
Treatment?
My model is that this abnormality/symptom is caused by fibrin or fibrin like deposit that prevents delivery of oxygen to brain tissue. How to deal with this? IMHO Fibronolytics are a start.
- https://cfsremission.wordpress.com/2012/12/30/bromelain-the-first-fibronolytic/
- https://cfsremission.wordpress.com/2012/12/31/nattokinase-2nd-choice-for-fibrinolytics/
- https://cfsremission.wordpress.com/2013/01/01/serrapeptase-3-choice-for-fibrinolytics/
- https://cfsremission.wordpress.com/2013/01/02/lumbrokinease-the-4th-choice-for-fibrinolytics/
Bottom Line
With the microbiome shift as the maintainer (not cause) of CFS/FM/IBS, the difference in brain scans likely depends on how the shift happens on an individual patient. A 2017 study found that CFS without IBS, CFS with IBS can be reliably determine from critical shifts of just a few bacteria families. Similarly, Dr. Mayer reported in May 2017, that “For people with IBS research shows for the first time that there is an association between the gut microbiota and the brain regions involved in the processing of sensory information from their bodies. The results suggest that signals generated by the brain can influence the composition of microbes residing in the intestine and that the chemicals in the gut can shape the human brain’s structure.” [2017]
What we really need is a study done where:
- Each of the above scans are done on a group of patients, with their microbiome done at the same time.
- Neurological testing at the same time would be a nice to have
- Every year this is repeated.
- All of the data is pushed thru big data/ai analysis and we identify which bacteria causes which shifts on which scans…
