I have had to deal with a neurologist — fortunately I walked into the appointment with a SPECT scan that a radiologist had read as early Alzheimer’s (I was having severe short term memory issues in the CFS flare when the SPECT was done). The session went well, he confirmed that the Alzheimer’s diagnosis was wrong and fortunately was familiar with CFS patients and deem it to be very real.
A reader wrote today
“Hello, could you please link the research that shows which masses of the brain loose brain matter. I need to show this to my neurologist or she won’t help me get a spect done 😦 “
Pub Med Studies that should interest Neurologists
This is a technical post intended for neurologists, not brain fogged CFS patients.
 From Lactate in the brain by ME Reseach UK
From Lactate in the brain by ME Reseach UK
- “Mean lateral ventricular lactate concentrations measured by (1)H MRSI in CFS were increased by 297% compared with those in GAD (P < 0.001) and by 348% compared with those in healthy volunteers (P < 0.001), even after controlling for ventricular volume, which did not differ significantly between the groups. Regression analysis revealed that diagnosis accounted for 43% of the variance in ventricular lactate. CFS is associated with significantly raised concentrations of ventricular lactate, potentially consistent with recent evidence of decreased cortical blood flow, secondary mitochondrial dysfunction, and/or oxidative stress abnormalities in the disorder." [2009]
- “Ventricular cerebrospinal fluid lactate was significantly elevated in CFS compared to healthy volunteers, replicating the major result of our previous study. Ventricular lactate measures in MDD did not differ from those in either CFS or healthy volunteers. ” [2010]
- ” We found elevated ventricular lactate and decreased GSH in patients with CFS and MDD relative to HVs. GSH did not differ significantly between the two patient groups. In addition, we found lower rCBF in the left anterior cingulate cortex and the right lingual gyrus in patients with CFS relative to HVs, but rCBF did not differ between those with CFS and MDD. We found no differences between the three groups in terms of any high-energy phosphate metabolites. In exploratory correlation analyses, we found that levels of ventricular lactate and cortical GSH were inversely correlated, and significantly associated with several key indices of physical health and disability. Collectively, the results of this third independent study support a pathophysiological model of CFS in which increased oxidative stress may play a key role in CFS etiopathophysiology.” [2012]
- “Less efficient and costly processes of frontal cortex in childhood chronic fatigue syndrome. [2015]
- “We conducted a study using a dual verbal task to assess allocation of attentional resources to two simultaneous activities (picking out vowels and reading for story comprehension) and functional magnetic resonance imaging. Patients exhibited a much larger area of activation, recruiting additional frontal areas. The right middle frontal gyrus (MFG), which is included in the dorsolateral prefrontal cortex, of CCFS patients was specifically activated in both the single and dual tasks; this activation level was positively correlated with motivation scores for the tasks and accuracy of story comprehension. In addition, in patients, the dorsal anterior cingulate gyrus (dACC) and left MFG were activated only in the dual task, and activation levels of the dACC and left MFG were positively associated with the motivation and fatigue scores, respectively. Patients with CCFS exhibited a wider area of activated frontal regions related to attentional resources in order to increase their poorer task performance with massive mental effort.”
MRI:
-
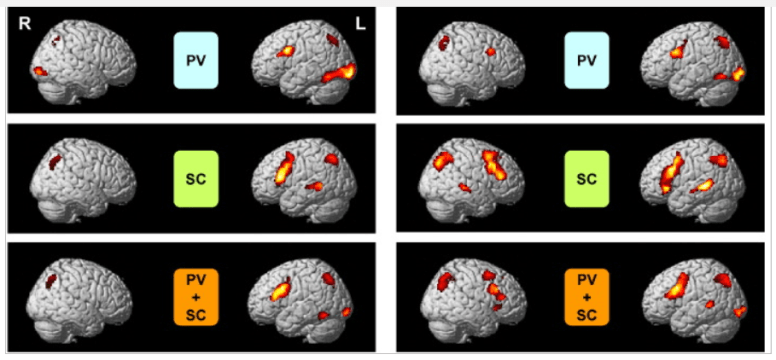
- “This study investigated responses to acute tryptophan feeding (after administration of 30 mg/kg body mass) using functional magnetic resonance imaging to investigate neural correlates of central fatigue during a cognitively demanding exercise, the counting Stroop task. Thus, tryptophan administration before the Stroop task caused distributed functional changes in primary sensory and in multimodal neocortex, including changes in a brain region, the activity of which has been shown previously to vary with conscious awareness (precuneus). Previous reports suggest that primary mechanisms of central fatigue may be predominantly subcortical. The present results demonstrate that neocortical activity changes are also found” [2007]
- “The primary purpose of the study was to use functional magnetic resonance imaging (fMRI) to determine Results showed that mental fatigue was significantly related to brain activity during the fatiguing cognitive task but not the finger tapping or simple auditory monitoring tasks. Significant (p< or =0.005) positive relationships were found for cerebellar, temporal, cingulate and frontal regions. A significant (p=0.001) negative relationship was found for the left posterior parietal cortex. CFS participants did not differ from controls for either finger tapping or auditory monitoring tasks, but exhibited significantly greater activity in several cortical and subcortical regions during the fatiguing cognitive task." [2007]
- “In a series of two Blood Oxygen Level Dependent (BOLD) functional Magnetic Resonance Imaging (fMRI) studies, … Within and between regions of interest (ROI), group analyses were performed for both studies with statistical parametric mapping (SPM99). Findings showed that individuals with CFS are able to process challenging auditory information as accurately as Controls but utilize more extensive regions of the network associated with the verbal WM system. Individuals with CFS appear to have to exert greater effort to process auditory information as effectively as demographically similar healthy adults.” [2005]
- Right arcuate fasciculus abnormality in chronic fatigue [2015]
- “Bilateral white matter atrophy is present in CFS. …Right hemispheric increased FA may reflect degeneration of crossing fibers or strengthening of short-range fibers. Right anterior arcuate FA may serve as a biomarker for CFS.”
SPECT:
- “Radiological imaging studies (SPECT, Xe-CT, and MRS) revealed decreased blood flow in the frontal and thalamic areas, and accumulation of choline in the frontal lobe.” [Learning and memorization impairment in childhood chronic fatigue syndrome manifesting as school phobia in Japan. 2004]
- ” Regional blood flow studies by single photon-emission computerized tomography (SPECT) have been more consistent. They have revealed blood flow reductions in many regions, especially in the hind brain. Similar lesions have been reported after poliomyelitis and in multiple sclerosis–in both of which conditions chronic fatigue is characteristically present. In the well-known post-polio fatigue syndrome, lesions predominate in the RAS of the brain stem. ” [Chronic fatigue syndrome–aetiological aspects. 1997]
- ” Patients with chronic fatigue syndrome had significantly more defects throughout the cerebral cortex on SPECT scans than did normal subjects (7.31 vs 0.43 defects per subject, p < .001). SPECT abnormalities were present in 13 (81%) of 16 patients, vs three (21%) of 14 control subjects (p < .01). SPECT scans showed significantly more abnormalities than did MR scans in patients with chronic fatigue syndrome(p < .025).” [Detection of intracranial abnormalities in patients with chronic fatigue syndrome: comparison of MR imaging and SPECT. 1994]
- “Compared with the Normal Control group, the CFS group showed significantly lower cortical/cerebellar rCBF ratios, throughout multiple brain regions (P < 0.05). Forty-eight CFS subjects (80%) showed at least one or more rCBF ratios significantly less than normal values. The major cerebral regions involved were frontal (38 cases, 63%), temporal (21 cases, 35%), parietal (32 cases, 53%) and occipital lobes (23 cases, 38%). The rCBF ratios of basal ganglia (24 cases, 40%) were also reduced.” [Assessment of regional cerebral perfusion by 99Tcm-HMPAO SPECT in chronic fatigue syndrome. 1992]
Brain Matter Volume
These was the requested studies asked for by the reader. I cite the 2015 studies that links to six earlier studies.
- Gray matter volumes in patients with chronic fatigue syndrome [2015].
- “Although most studies found Gray Matter volumes reduced in some brain regions in CFS, as we discussed above, there are so many factors that could affect brain structure should have been considered. So far, no study has controlled all these factors.”
- We found 6 studies focusing on the change of GM volumes. Okada et al. [34] found in a voxel-based morphometric study of CFS that GM volumes reduced in bilateral prefrontal and that the affected areas extended from Brodmann area (BA) 8 to 9 in right cerebral hemisphere and from BA 9 to 11 in left. Puri et al. [35] also found that GM declined in occipital lobe, right angular gyrus, and posterior division of the left parahippocampal gyrus in a voxel-based morphometric 3-T MRI study. de Lange et al. [36] found that global GM volumes reduced by 8% compared to healthy controls and the rate of decline is 2.2 mL/year in a cohort study; moreover, the GM volumes could increase after cognitive behavioral therapy [37].
Bottom Line
CFS/ME alters the brain in many ways. Many of the alterations correspond to symptoms.