
I have just finished doing a bunch of deep dives of some of the bacteria genus that are high in CFS. This makes it faster to do an analysis. Most of the information about probiotics impact was published in 2017, a little in 2016. I expect many more studies in 2018. As new information comes in, recommendations will evolve.
The working hypothesis is that the high genus are causing many symptoms. CFS have many symptoms — so different high genus are expected. This makes effective treatment more difficult for CFS as a group; in theory with uBiome results we can individualize treatment for the person’s uBiome shifts.
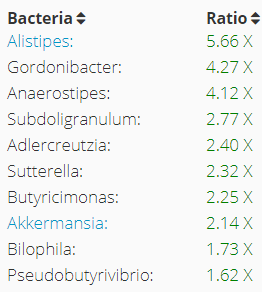
Similar uBiomes with high (Butyricimonas, Alistipes, Gordonibacter)
- https://cfsremission.wordpress.com/2017/08/23/treatment-options-for-a-ubiome-subset/
- https://cfsremission.wordpress.com/2017/09/03/ubiome-result/
- https://cfsremission.wordpress.com/2017/09/18/more-before-and-after-fecal-microbiome-transplants-ubiomes/
The original analysis was done in June 2017, in this post. The old advise was “Resume with heavy dosages of Bifidobacterium, Consider adding some Lactobacillus (see this post)“. In this post specific strains to take or avoid are derived from these new studies.
Basics:
Bifidobacterium: 0x, Lactobacillus: 0.02x, Enterobacteriaceae (E.Coli parent) 0x, Akkermansis 2.97x, Firmicutes to Bacteroidetes: 1.4::1 (Normal 2.1::1)
- Alistipes: https://cfsremission.wordpress.com/2017/10/09/decreasing-alistipes-genus/
- Gordonibacter: https://cfsremission.wordpress.com/2017/10/09/decreasing-gordonibacter-genus/
- Anaerostipes: https://cfsremission.wordpress.com/2017/10/07/decreasing-anaerostipes-genus/
- Subdoligranlum: https://cfsremission.wordpress.com/2017/10/10/decreasing-subdoligranlum/
- Adlercreutzia: https://cfsremission.wordpress.com/2017/10/14/decreasing-adlercreutzia-genus/
- Sutterella: https://cfsremission.wordpress.com/2017/10/13/decreasing-sutterella-genus/
- Butyricimas: https://cfsremission.wordpress.com/2017/10/14/decreasing-butyricimonas-genus/
- Akkermansia: https://cfsremission.wordpress.com/2017/10/14/decreasing-akkermansia-genus/
- Bilophila: https://cfsremission.wordpress.com/2017/10/14/decreasing-bilophila-genus/
- Pseudobutyrivibrio: https://cfsremission.wordpress.com/2017/10/15/decreasing-pseudobutyrivibrio-genus/
Rare Bacteria ( <5%)
Bottom Line
The following is derived from the research consolidated above. It is a logical inference (theoretical) that have not been tested in human studies on patients with any autoimmune like diseases.
THIS IS NOT A GENERAL RECOMMENDATION FOR ALL CFS PATIENTS. It is specific to one person with their unique-to-them ubiome. It’s purpose is show that uBiome results may point to specific probiotics.
Food
Inconclusive:
Take
- Cranberry bean flour (or fresh cranberries)
- Tannin and Gallate — green tea see this web page.
- Vitamin K2 (Menaquinone-7 etc)
- Grapes (table) – likely grape seed extract will help
Avoid
- Pomegranate and walnuts
- Raspberries
- Omega 3
- Berberine
- Black tea
Probiotics
Take
Ideally without inulin or other prebiotics
- E.Coli Nissle – Mutaflor and Symbioflor-
- Lactobacillus kefiri
- Lactobacillus paracasei
- Lactobacillus plantarum
- Lactobacillus rhamnosus GG
- Streptococcus probiotics
Avoid
- Bifidobacterium Adolescentis
- Bifidobacterium animalis subsp. lactis (B-12®)
- Bifidobacterim Breve
- Bifidobacterium Longum.
- Clostridium butyricum (i.e. Miyarisan)
- Lactobacillus Casei
- Lactobacillus Salivarius
- Saccharomyces boulardii
Addendum
From some reader feedback, the lists above can exceed the band width of the CFS fogged brain. My general advice on how to implement the above is based on the concept
“Haste looses information and create uncertainty“
CFS patients want to rush to remission and in so doing they overload on supplements and some item makes it worst. They will arbitrary ascribe it to one of the items and often pick the less likely one. The following is how I would proceed for myself.
- Step #1 if you have any probiotics on the AVOID list that you are actively taking — keep taking them until you have a week supply left, then stop them. We want to retry them later (remember the above is in theory)
- Step #2 As each probiotic goes to the pause state, add in one of the new TAKE probiotic (no more than 1/week), slowing increase the dosage. Be aware of costs (work from the cheapest). Ideally 10-30 BCFU of each. CustomProbiotics.com can be as cheap as 5 cents for 10 BCFU to $0.79 for 10 BFCU for align if fresh from the factory (or $79 BCFU if close to use by date on package)
- Stop any supplements on the AVOID list. Give yourself 5 days to wash out — if you crash, then return them and try isolating out the ones you really need.
- After a 5 day wash out, start adding in new ones (no more than 1 new one a week). See if you can determine “recommended daily allowance”(Lowest level) and “Highest accepted as safe level”
- You want therapeutic levels, which means high levels, slowly worked up
- Example: Vitamin K2 cited above:
- Search using https://www.ncbi.nlm.nih.gov/pubmed/?term=vitamin+K2+dosage
- “Low dosage… up to 200 μg menaquinone-7 daily for 4 wk, ” [2015]
- “The tolerable upper intake level (UL) was determined for vitamin A, vitamin D and vitamin E, but not for vitamin K, since no adverse effects have been reported even with its high dosage.” [2010].
- When there is no known upper limit, I usually assume that 2-3x a known safe lower limit should be fine.
- For food, teas, etc … start shifting your diet away from the AVOID and try to have at least one TAKE every couple of days at least. For teas, a cup with each meal would be a reasonable goal.
This is a personalized addition based on an individual’s ubiome results. It is in addition to the general theoretical guidance provided in this post.
This is an education post showing how ubiome results could lead to specific recommendations to reduce high bacteria genus. Always consult with a medical professional before starting or stopping probiotics, supplements etc.
