
Fecal transplants for CFS/IBS etc typically result in almost immediate resolution of symptoms — followed weeks or months later with relapse. Fecal transplant for Clostridium difficile has a high persistent success rate. (“of the approximately 200 cases reported, regardless of route, a mean success rate of 96% has been achieved.27” [2011])
So why the difference? In one case we are talking of displacing a single bacteria species (C. difficile); in the CFS case, we are having to both replace/reduce multiple strains AND restart other strains.
Determining suitable donor to match the patient
For C.difficile — any apparently healthy donor (i.e. does not have C. difficile) is a viable candidate.
For CFS, the donor criteria should be:
- Normal levels of
- Lactobacillus
- Bifidobacterium
- E.Coli
- Akkermansia
Matching uBiome profiles
It should be apparent that the donor should not have any bacteria genus > 1.5x that the recipient has > 1.5x.
Updated: “No bacteria genus > 1.5x should be on the list of common bacteria genus overgrowths listed at Overview of this Blog and the Microbiome.“
Ideally, at the strain level (of any existing bacteria of the recipient) — Lactobacillus, Bifidobacterium and E.Coli should be extremely close matches.
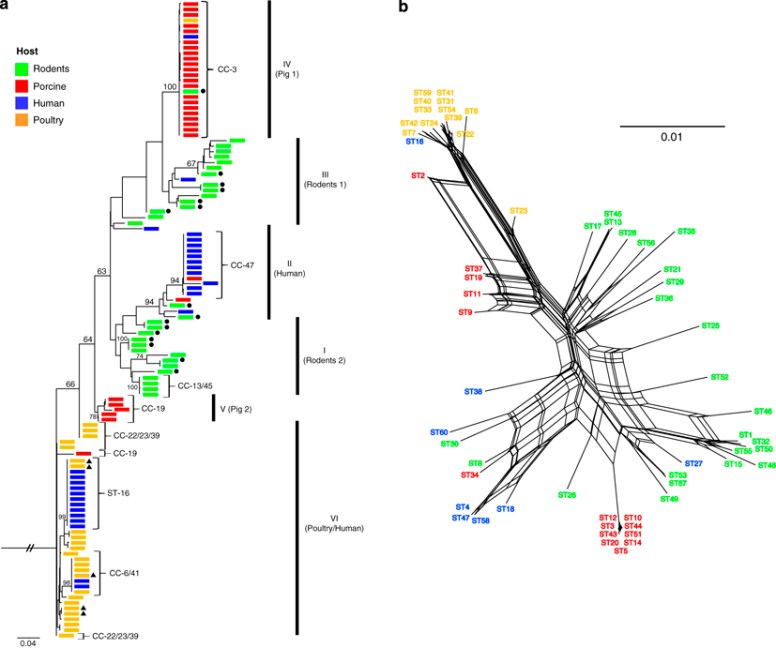
To illustrate this aspect, examine this chart of L.Reuteri strains [Source 2009]
Pre-Transplant Preparation
6 weeks before the transplant, the recipient should be on a probiotic and diet regime based on their own uBiome to reduce the over growth.
Track microbiome shift immediately before and after transplant
To better improve the transplant method, I would advocate the following uBiome (or equivalent) samples be taken:
- Two days before transplant of both recipient and donor (or on donation day)
- Two, four, eight, sixteen, thirty-two, sixty-four days after the transplant
Recipient should keep on the probiotic and diet regime based on their own uBiome for at leasy 30 days after the transplant.
Logic: We want to suppress the overgrowth before the transplant and keep it suppressed while the transplant gets established.
To the best of my research, I have not seen any studies tracking the microbiome regularly after a transplant…. there appear to be process happenings with the failures that we need to understand better.
Again, this is just a theoretical protocol applying logic to known facts.
