A reader asked me to compile a list of of published studies and articles on the use of antibiotics with ME/CFS. Note that with gut dysbiosis as the model, the choice of antibiotics may depend on the details of the dysbiosis (this a 16s or shotgun GI report is suggested. Xenogene.es offers excellent reports).
At the Whittemore Peterson Institute (WPI) is a non-profit medical research institute dedicated to the support of those with a spectrum of neuro-immune diseases (NIDs) including: myalgic encephalomyelitis, (ME), fibromyalgia, and similar complex chronic diseases of the immune system and the brain. Dr. De Meirleir earned his medical degree from the Vrije Universiteit Brussel in 1977, and completed an internal medicine residency in the Department of Internal Medicine, University Hospital of Vrije Universiteit Brussel. His current research focuses on a subgroup of ME patients who show evidence of chronic bacterial infection and gut dysbiosis. These patients are responding to specific antibiotic/ probiotic therapy.
http://nvcbr.org/portfolio-items/kennydemeirleir/
- Azithromycin in Chronic Fatigue Syndrome (CFS), an Analysis of Clinical Data (2006) ” Results: Of the 99 patients investigated, 58 reported a decrease in the symptoms by the use of azithromycin.”
- Open-label Pilot for Treatment Targeting Gut Dysbiosis in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Neuropsychological Symptoms and Sex Comparisons (2018) ” Large treatment ( alternate weeks of Erythromycin (400 mg of erythromycin as ethyl succinate salt) twice daily ) effects were observed for the intention-to-treat sample with a reduction in Streptococcus viable count and improvement on several clinical outcomes including total symptoms, some sleep (less awakenings, greater efficiency and quality) and cognitive symptoms (attention, processing speed, cognitive flexibility, story memory and verbal fluency). “
- Chronic Fatigue Syndrome After Q Fever (2007) ” After 4-12 months they developed post-Q-fever fatigue syndrome and were treated with intracellular active antibiotics (fluoroquinolones and tetracycline) for 3-12 months. Efficacy of the treatment was observed in two patients, but in one patient the results were not encouraging. “
- Sleep Quality and the Treatment of Intestinal Microbiota Imbalance in Chronic Fatigue Syndrome: A Pilot Study (2015) ” Participants were administered erythromycin 400 mg b.d. for 6 days… Short term antibiotic treatment appears to be insufficient to effect sustainable changes in the gut ecosystem in most CFS participants. Some improvement in objective sleep parameters and mood were found in participants with reduced levels of gram-positive gut microbiota after antibiotic treatment, which is encouraging. Further study of possible links between gut microorganisms and sleep and mood disturbances is warranted. “
- On the Question of Infectious Aetiologies for Multiple Sclerosis, Schizophrenia and the Chronic Fatigue Syndrome and Their Treatment With Antibiotics (2009)… ” in the beginning of 2007 two female patients suffering from severe and long standing chronic fatigue syndrome were added. The first of them, after sixty days of treatment with antibiotics showed excellent treatment results on follow-up one year later, whereas the second, who also took the combination of antibiotics for sixty days, was rated as having shown a significant improvement. “
- Mycoplasma Blood Infection in Chronic Fatigue and Fibromyalgia Syndromes (2003) ” Most patients with CFS/FMS who have mycoplasma infection appear to recover and reach their pre-illness state after long-term antibiotic therapy with doxycycline, and the infection can not be detected after recovery. “
- ” Dr. Nicolson suggests long-term antibiotic treatment with drugs such as doxycycline, cyprofloxacin, azithromycin, or clarithromycin. By long-term he means a continuous 6-month course of antibiotics followed by multiple 6-week cycles. The extended antibiotic treatment is needed because of “the intracellular locations of mycoplasmas… the slow-growing nature of these infections, their inherent insensitivity to most antibiotics and the persistence of the infections in metabolically inactive forms.” [Src]
- Role of Rickettsiae and Chlamydiae in the Psychopathology of Chronic Fatigue Syndrome (CFS) Patients (2000) Results: Group one: 79.5% good and very good results; 4.1% fairly good; 16.4% failed. Group two: 82.3% good and very good results; 2.5% fairly good; 15.2% failed. … All of the Dr. Bottero’s therapeutic results are confirmed since 1991 by Dr. Cecile Jadin of Randburg (South Africa) for more than 3000 CFS and other psychopathological states (300): Sydney 98 CFS Conference, Australia.
A treatment plan (Cecile Jadin’s is similar)
Treatment with antibiotics is difficult because drugs have to penetrate the host cell wall as well as the intracellular organisms. Treatment needs to be prolonged and pulsed, because of continual replication of the intracellular forms. Until adequate diagnostic facilities are readily available treatment needs to be in two stages: the first stage, which is diagnostic, involves the use of two long-term bacteriostatic antibiotics for 6 weeks, and the second, meant to be curative, involves the introduction of a third bactericidal antibiotic.
One possible choice of antibiotics for the first stage is a combination of Doxycycline and Azithromycin. Initially, the Doxycyline needs to be given alone in low dosage for two weeks, because of the risk of a Herxheimer reaction resulting from the release of toxins by damaged bacteria. Such reactions are usually mild and short-lived. If stable after two weeks, Azithromycin in low dosage is added for 4 weeks. Roxithromycin can be used in place of Azithromycin. . Improvement of symptoms, or the occurrence of a Herxheimer reaction, confirms the diagnosis.
Chronic fatigue syndrome or myalgic encephalomyelitis (2007) in British Medical Journal
From Published Books
By Erica Verrillo 2002

Bottom Line
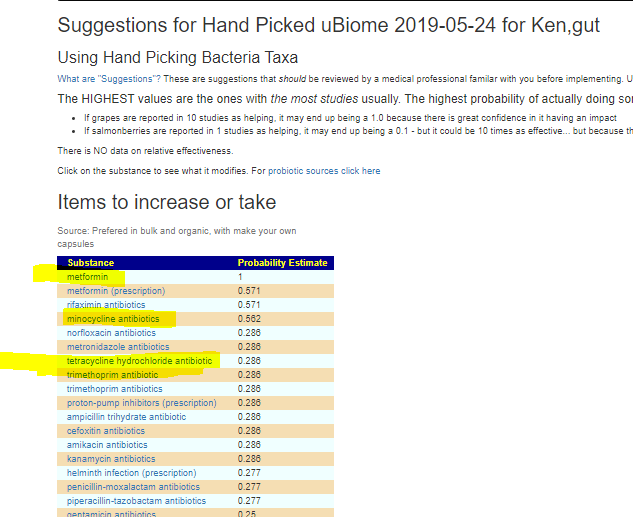
There is a high success rate reported with antibiotics. Recent research suggests that the failures may be selection of inappropriate antibiotics for the person’s specific gut dysbiosis. IMHO, a 16s or shotgun (Xenogene) microbiome report should be done and carefully analyzed prior to selecting the various antibiotics needed.
The microbiomePrescription site supports evaluation of antibiotics against a microbiome, as well as other prescription drugs.
Unfortunately, there has been only one comprehensive study done, so relative ranking may not apply for many samples (i.e. do a show all and scan for the ones that are most acceptable)
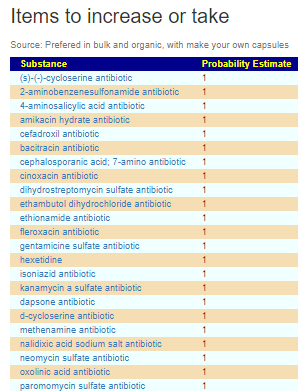
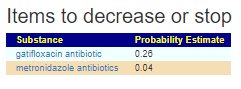
With hand-picking against ME/CFS profiles, results can get quite good. All of the antibiotics involved with prior successful treatment were listed.