
A reader wrote me asking about the different theories of ME/CFS, and I just read Cort’s The Best, the Most, the Strangest and the Worst of 2019 in ME/CFS and Fibromyalgia. I have used different models over the years (going with the best available usually). Often it seems that both patients and researchers are lost in the forest strictly following a compass bearing and crossing over paths (and ignoring) that may lead them out of the forest.
My academic training is modelling. A model is a hypothesis with some extra criteria:
- Must be predictive
- Must be testable
- Must explain existing observations
- Should be as simple as possible
A good model is one that explains more observations than other models. A good model is one that is easy to test. A good model predicts possible findings (which if the findings comes in correct, confirms the model).
The most challenging set of observations
The following is known to every ME/CFS patient and treating physician: The huge variation of symptoms. For a list of non-lab symptoms, see MEpedia Page, CDC Page, Review of the Evidence on Other ME/CFS Symptoms and Manifestations, and Review of the Evidence on Major ME/CFS Symptoms and Manifestations.
We know that DNA/SNP plays a role – for example, ME/CFS people have smaller hearts, craniocervical instability and certain DNA mutations are more common. These are not causes (people with the same items do not have ME/CFS) but contributing factors that makes people more disposes to developing ME/CFS. Think of the “Perfect Storm”, you have a sea worthy boat — unfortunately you motor died in the middle of gale when you were close to a reef…. a series of unfortunate events.
My criteria for a hypothesis that has merit to investigate or fund — it must give an explanation for the different symptoms! A common response is there are different subsets and we need to identify each subset first, or ‘we have not had time to investigate that yet’ (and likely will never) or even a truthful, “I don’t know” or perhaps a dismissive “that’s not relevant”.
The Microbiome Model explains Symptoms
A rhetoric question — if all of your ME/CFS symptoms disappear do you have ME/CFS. At one time remission was defined as no longer having the minimum number of symptoms required for the CDC definition.
About a seven months ago, I tossed up an analysis page on symptoms to bacteria expecting weak results. I was shocked, Eureka! Specific bacteria are associated with specific conditions and symptoms. Since then the database have grown and the number of people entering symptoms have increased.
Alcohol Intolerance
This occurs in a very high percentage of M/E CFS patients. Our analysis found that there were specific microbiome shifts (high levels of certain bacteria)
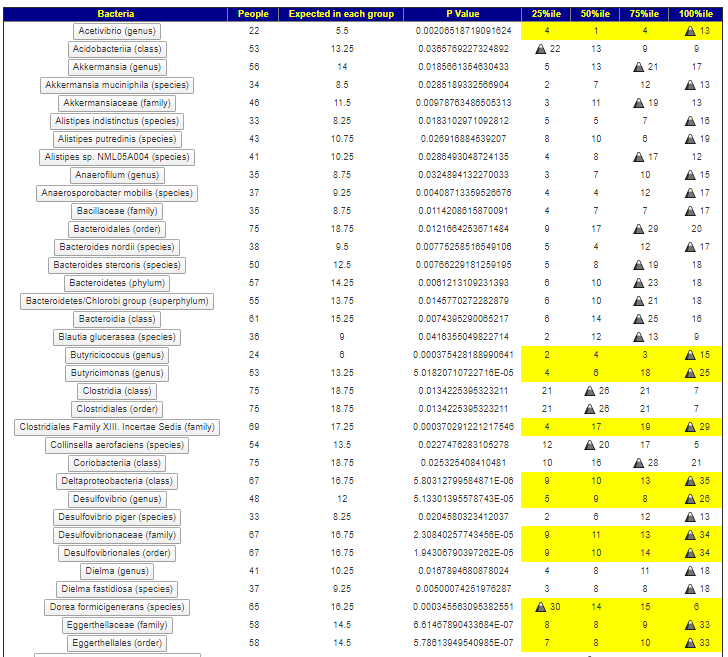
Neurological: Difficulty reading
We find similar patterns, and can drill down to higher resolution (because of more data) and see a strong clustering with people with the highest 15% of some bacteria.
Neurocognitive: Difficulty paying attention for a long period of time
As we walk thru them, we notice overlaps of some bacteria. Look at what is below and alcohol intolerance above. We see the following in common
- Butyricimonas (genus)
- Deltaproteobacteria (class)
- Desulfovibrionales (order)
These are the main players for some ME/CFS, the other bacteria likely cooperate with them to produce specific symptoms (which often have a DNA requirement to appear).
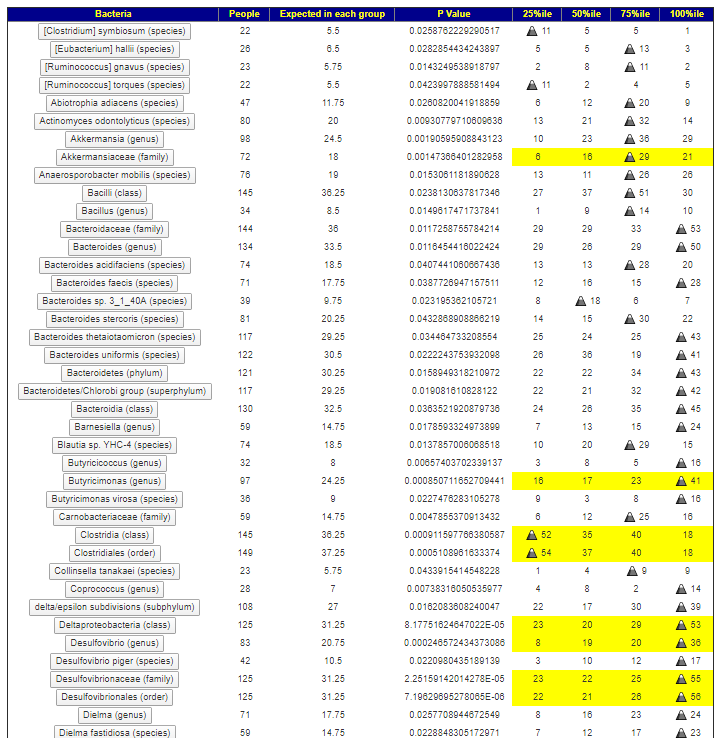
I should point out that a P-value of 0.05 or below is often the criteria for getting a finding published in a medical journal. Some of the values we came up with are 0.000194 and lower. Much much stronger evidence than is usually seen.
Summary
The criteria are below:
- Must be predictive
- Must be testable
- Must explain existing observations
- Should be as simple as possible
The microbiome model beats everything else (please add detail comments if you disagree of which model is better using these criteria).
This model is predictive, it can take a microbiome sample in and based on the content alone predict probable symptom (key word is probable) which from my own experience and other user feedback seems around 75% accurate.
This mode is testable, from a microbiome sample we can determine a list of items that would probably help. Some people have had outstanding results. Again, the key word is probable.
This model explain existing observations, the observations we used above in symptoms. Recent research studies also find that it explains many lab results seen with ME/CFS.
This model is simple to understand. It is a beast to work with because of the number of bacteria involved.
The last issues for me are treatment-actionable and available. Most of the research hypothesis do not have treatments to address the cause. A few that do are usually not available — often because it is a research protocol and not “standard of medical care” .. i.e. no one can use, especially the ordinary family physician sitting in a community clinic in the Australian Outback!
The microbiome can be manipulated without prescription drugs which removes the stumbling block of “standard of medical care”. It can even be done under quasi-medical supervision if a patient uses available tools and present the suggestions to their physician for review. Getting physicians up to speed on the microbiome is a different issue.
If you believe a different model is better — then please provide the details in the comments. I am open to changing models.
