The person in this prior post has done a retest. This analysis looks at what changed from selectively following suggestions from this prior post.
- ME/CFS Follow Up Microbiome Samples
- Follow up Microbiome Analysis from a prior post
- Rosacea, Circulation and mild CFS
His comments are below:
“Things that I have been taking since the last test in February 2023:
- Rosemary
- Grapefruit seed extract
- Turmeric
- Natto
- Tetracycline
- Clove
- Anise
- Acacia gum
- Amoxicillin
- Apple peel powder
- Thyme
- Symbioflor 2
- Neem
- Jarlsberg cheese
My symptoms:
- Still get the red nose (some form of rosacea). But it is better than before.
- Still feel fatigued (both physically and mentally). But it is better than before.
- Feeling stressed. But it is better than before.
- Brain fog.
- Bloated.
- Lots of gas – I fart and burps a lot. “
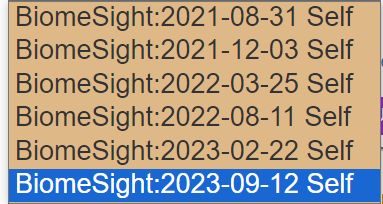
This is his fifth sample. Multiple samples are not unusual because fixing the microbiome means a lot of course corrections.
Analysis
First, we will look at measures that were not available for the earlier posts. In the last period, we see a dramatic change of the histamine values!
| Sample | Anti-Inflammation Value | Histamine Value |
| 2021-08-31 | 97%ile | 98%ile |
| 2021-12-03 | 96%ile | 98%ile |
| 2022-03-25 | 18%ile | 87%ile |
| 2022-08-11 | 30%ile | 90%ile |
| 2023-02-22 | 65%ile | 86%ile |
| 2023-09-12 | 87%ile | 3.2%ile |
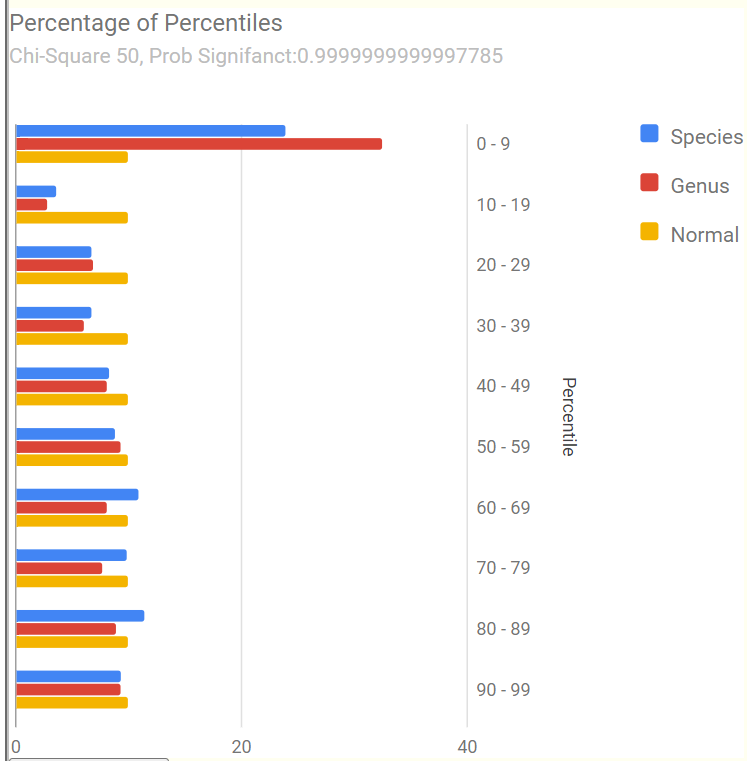
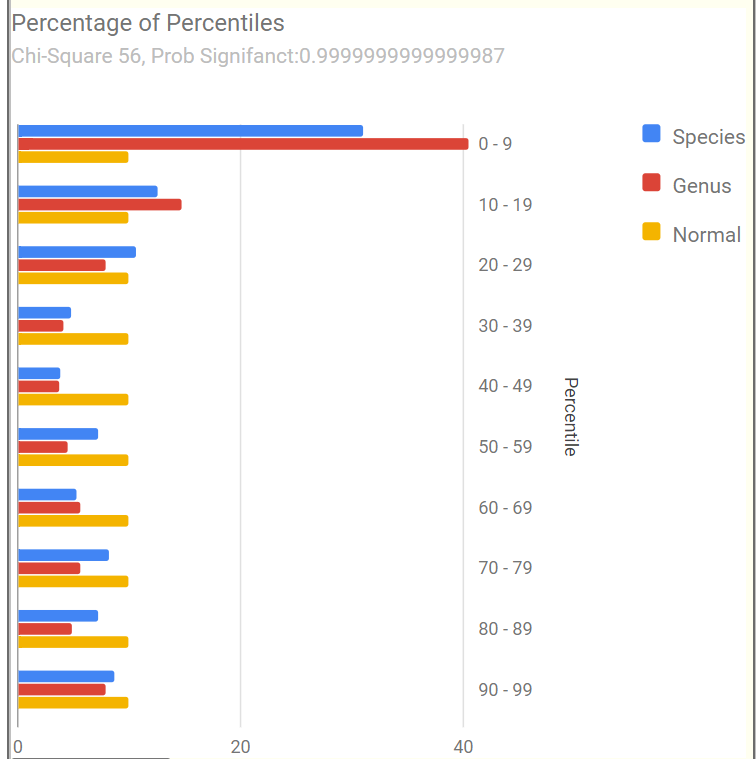
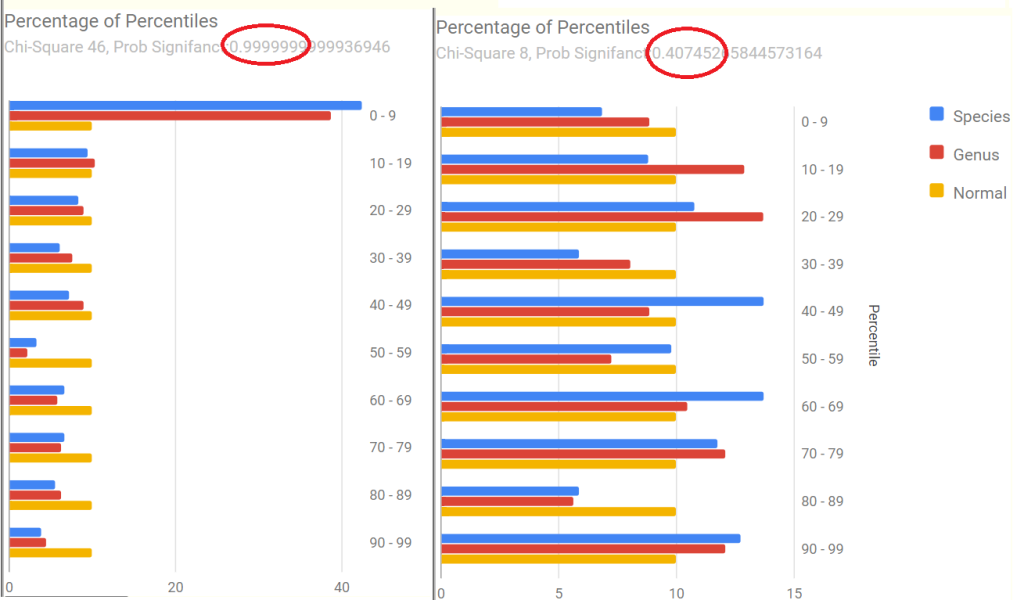
We also see a dramatic change in the Percentages of Percentiles charts that suggests improvement. In fact, there is no longer any statistically significant shifts (going from 0.99999… to .40!). Dropping below 0.95 is an objective target. The pattern went from the common ME/CFS and Long COVID pattern to an normal pattern.
Potential Medical Conditions Detected
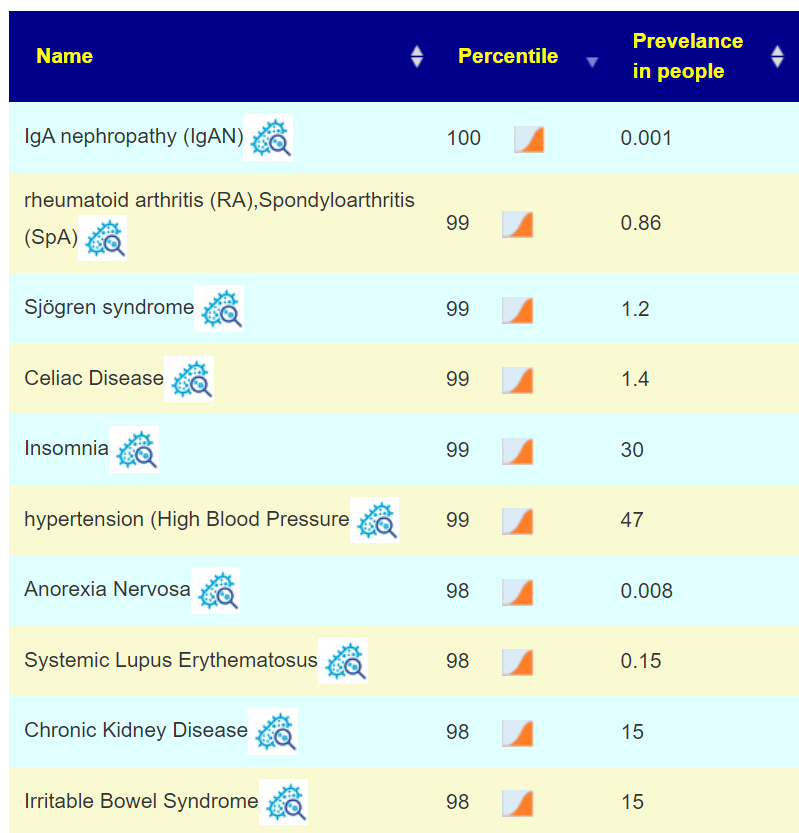
We have the following candidates to consider that were not flagged in the prior sample (where nothing stood out):
- Allergic Rhinitis (Hay Fever): 100%ile
- Stress / posttraumatic stress disorder: 98%ile
- Irritable Bowel Syndrome: 97%ile
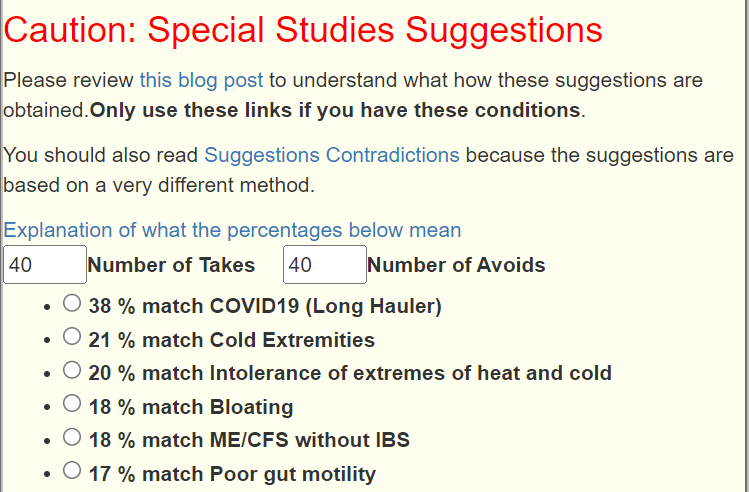
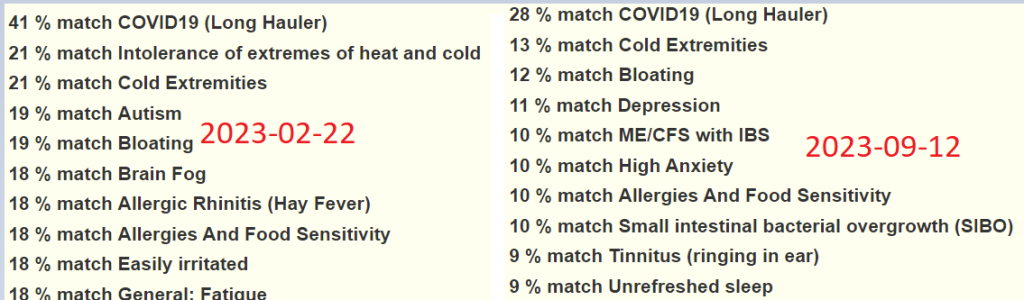
This may be just randomness or because the microbiome is calming down, patterns hidden by noise are showing up. Looking at Special Studies pattern matching, the top one was COVID19 (Long Hauler) at 28% match (prior was 41% match) — a definite improvement. Other items dropped about 8% match each, most were so low, that there may not be significance.
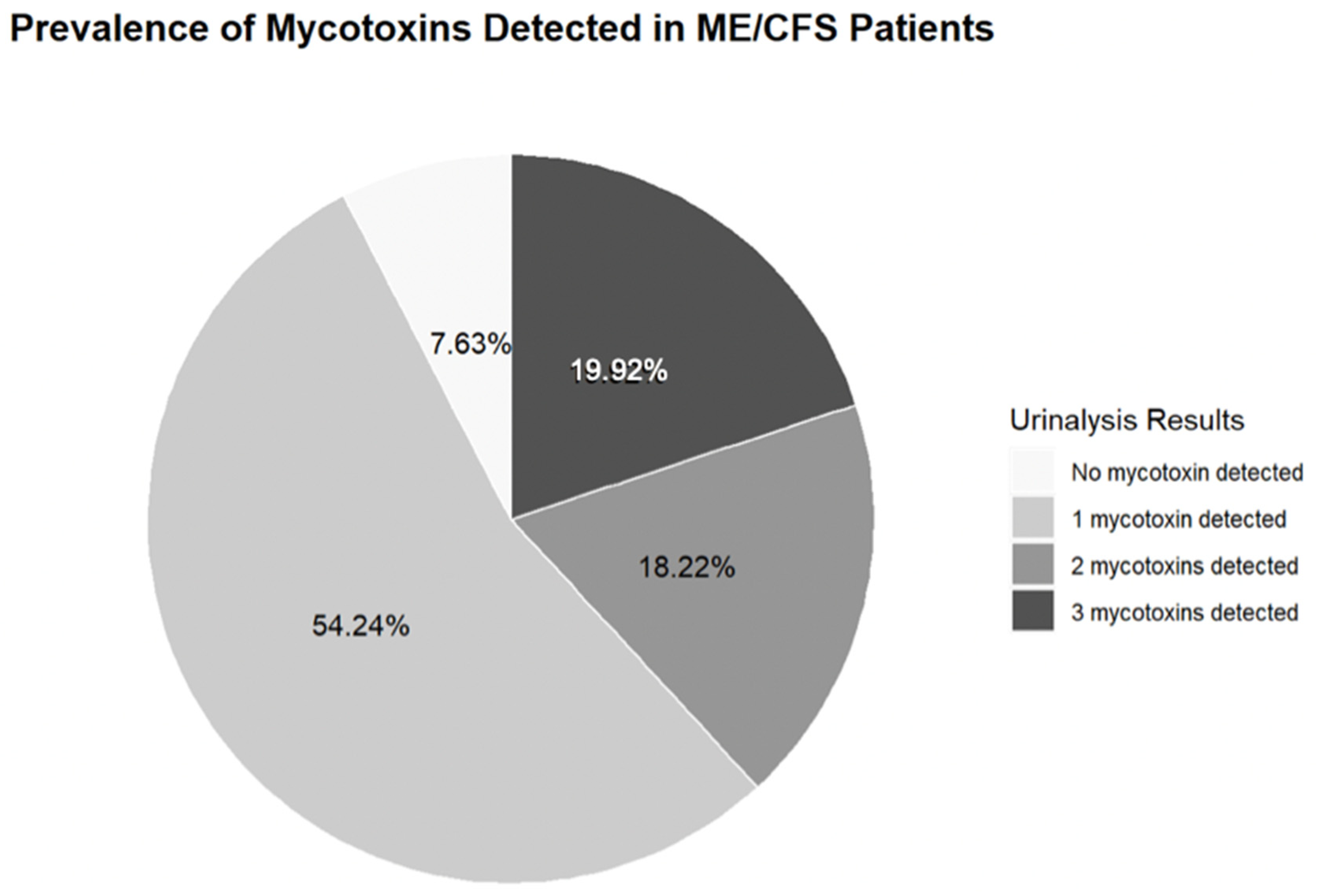
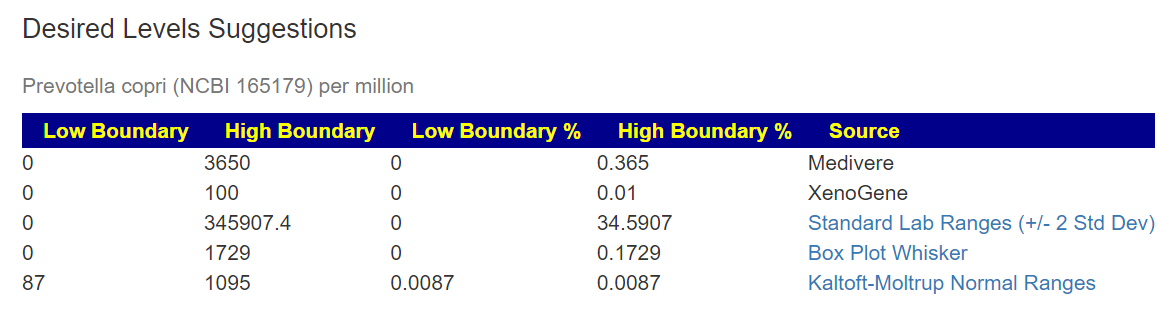
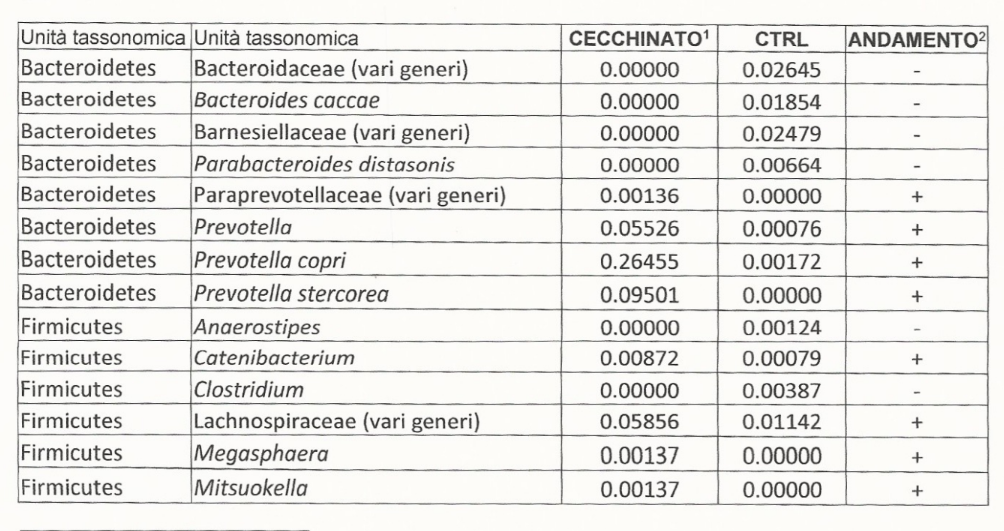
These appear to agree with his personal observations. We have Prevotella copri is at 76%ile, hinting that mycotoxin present (mold) may be in his environment (see this post for more exploration).
Going Forward
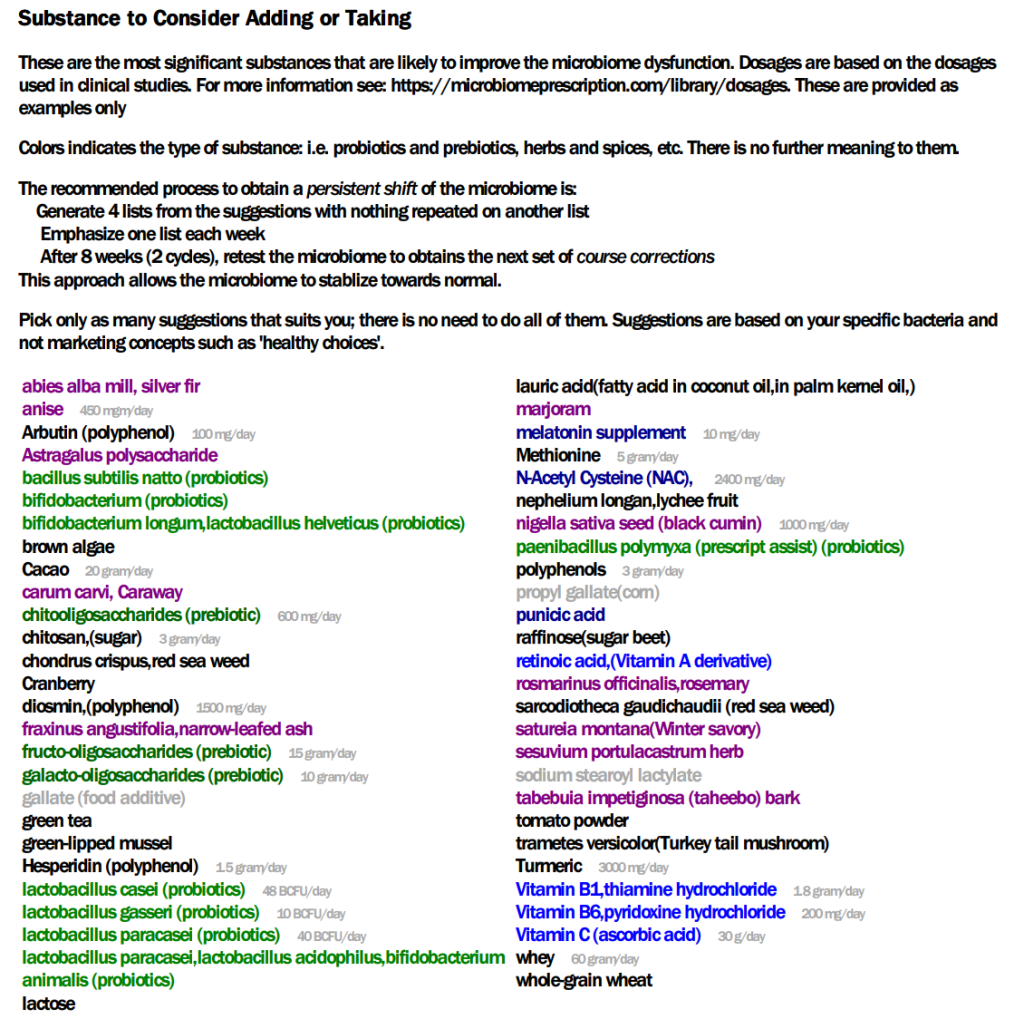
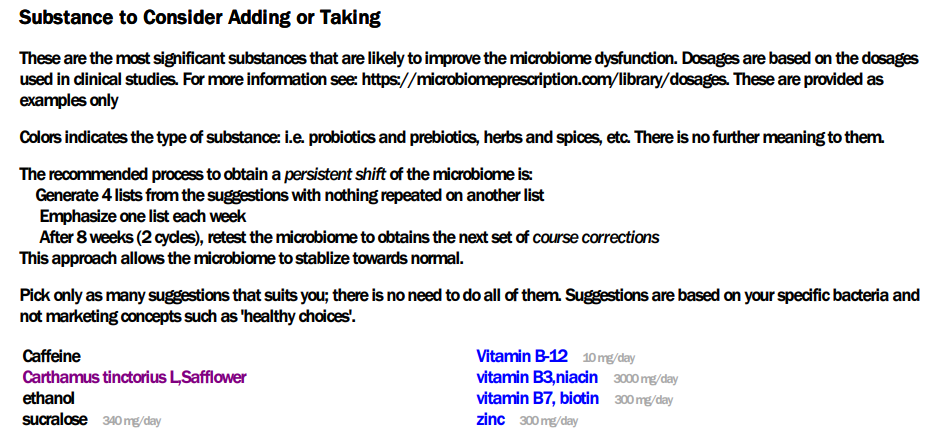
In terms of subjective and objective measurements, this person has improved. So time for the next course correction. I am going to just run with the “just give me suggestions” since nothing really stands out.
The non-prescription items from the PDF are by far the shortest that I have seen! So the safflower may be difficult because it does not mean safflower oil (an avoid), but the herb.lots of coffee and perhaps a little Aalborg Aquavit.
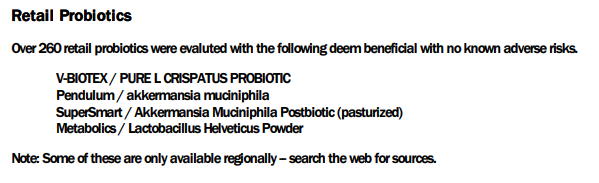
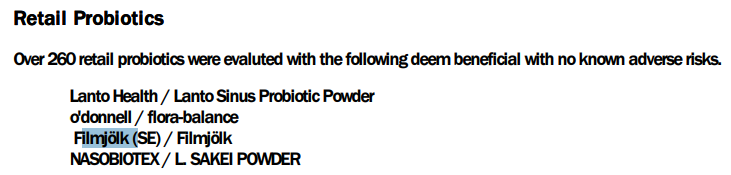
In terms of probiotics, he lucked out — Filmjölk is likely available to him
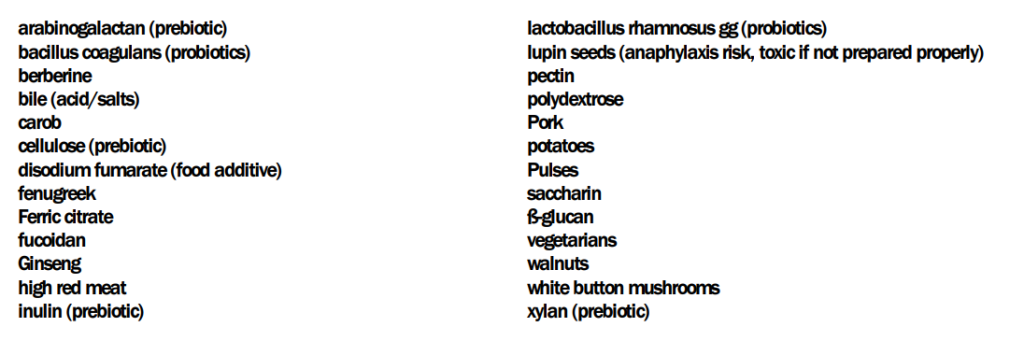
The avoid or reduce list is much longer!!
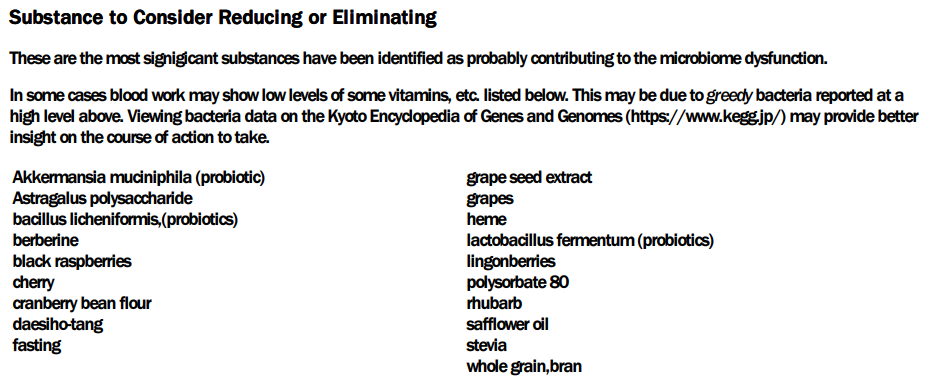
Going over to items computed from the Kyoto Encyclopedia of Genes and Genomes we have the top item being the typical one for ME/CFS: Escherichia coli (i.e. Mutaflor or Symbioflor-2). In terms of supplements, the two most significant one are: Glutamine, Threonine, Serine.
Since the person has a co-operative MD (i.e. two antibiotics were listed), I reviewed the prescription items. The top item was amoxicillin (antibiotic)s[CFS], which has already been used. We have gatifloxacin, ciprofloxacin (antibiotic)s[CFS], and clinafloxacin (antibiotic) which is a different family (a fluoroquinolones which has a lot of bad press). The next one worth considering is nadifloxacin (antibiotic): Nadifloxacin is a broad-spectrum quinolone antibiotic(in fluoroquinolones family) that has been approved for use in the treatment of acne vulgaris and skin infections. This may impact his rosacea. The next one down the list may be similar: fusidic acid sodium salt (antibiotic).
One factor to consider is that Cecil Jadin has been using fluoroquinolones for twenty years without seeing any adverse effects. The duration is only 10 days or less. Longer duration of use may be a significant factor. See this post and video for more information.
Questions
“All those antibiotics MUST be taken: after food ( not only water ) and without any dairy products. Patients must avoid sugar intake and some supplements(for example magnesium). Antibiotics should be taken in the morning and the evening. Patients must avoid sugar intake and supplements.”Cecile Jadin, MD Video Presentation of Dr. Jadin’s Current Protocol for ME/CFS, Q-Fever, Chronic Lyme and related conditions
Q: I’m going to do another round with amoxicillin.
— In Jadin’s presentation she says to only take it for 7 days, ain’t ok to take it for 14 days as we talked about before?
— Can’t I take other supplements like magnesium when I take antibiotics?
- A: The duration range of 7 – 14 days is, IMHO, fine. My main concern is long duration that can result in antibiotic resistance.
- The other supplements while taking antibiotics is a good question. Jadin indicated that some items should not be taken. My IMHO (keeping to best odds thinking) would be to stop most of them with a few exceptions. We do not know that much about supplement-antibiotics interactions. The exceptions are antibiotic potentiators (items that allows the antibiotic to get deeper into “tissue”. See Antibiotic Potentiators Against Multidrug-Resistant Bacteria: Discovery, Development, and Clinical Relevance [2022] and my 2019 post Potentiators: Often the difference between success and failure. These include the following:
- Bromelain
- Serrapetase
- Nattokinease
- Lumbokinease
- Word of warning: If there a herxing, it will get a lot worse!! so start on a Friday night (and consider a few vacation days after the weekend!)
- The other supplements while taking antibiotics is a good question. Jadin indicated that some items should not be taken. My IMHO (keeping to best odds thinking) would be to stop most of them with a few exceptions. We do not know that much about supplement-antibiotics interactions. The exceptions are antibiotic potentiators (items that allows the antibiotic to get deeper into “tissue”. See Antibiotic Potentiators Against Multidrug-Resistant Bacteria: Discovery, Development, and Clinical Relevance [2022] and my 2019 post Potentiators: Often the difference between success and failure. These include the following:
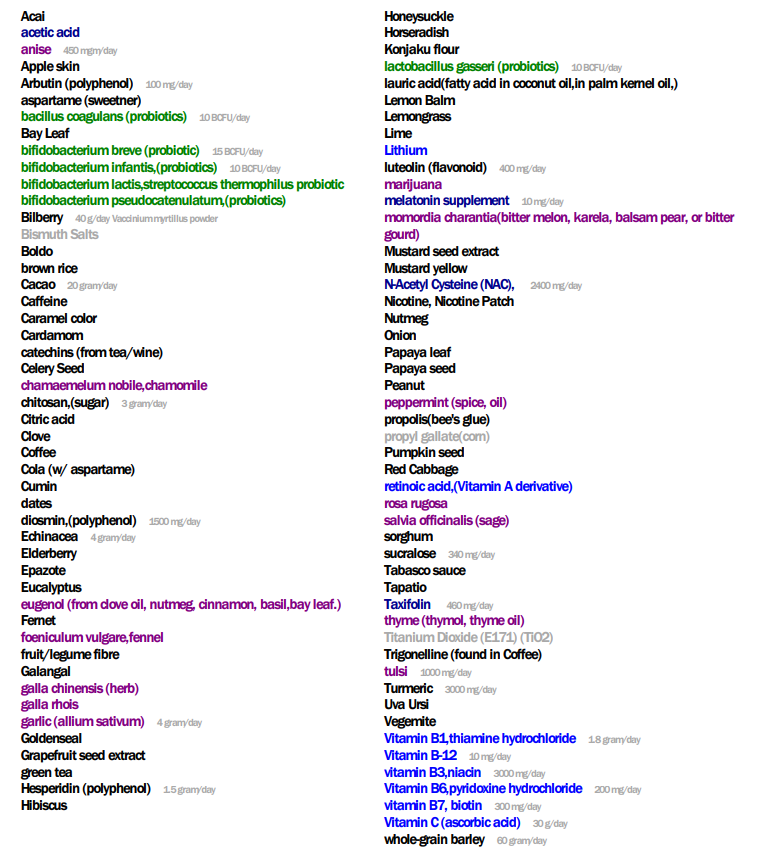
Q: If I want to have a longer list for what to take / avoid, can I use the three that is blue below (as earlier)?
- A: What is shown above is from the PDF which I am preferring to use for posts because it keeps things simpler. You can do any combination you wish. You could also consider doing your last sample suggestions and this sample suggestions, an “uber consensus” which should produce suggestions of what has been out of range with both samples. Caution should be done because of how different the two samples are!
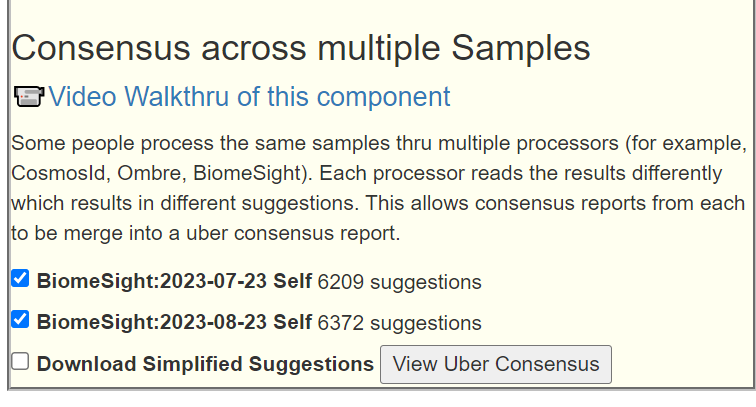
This does produce a massive list!!
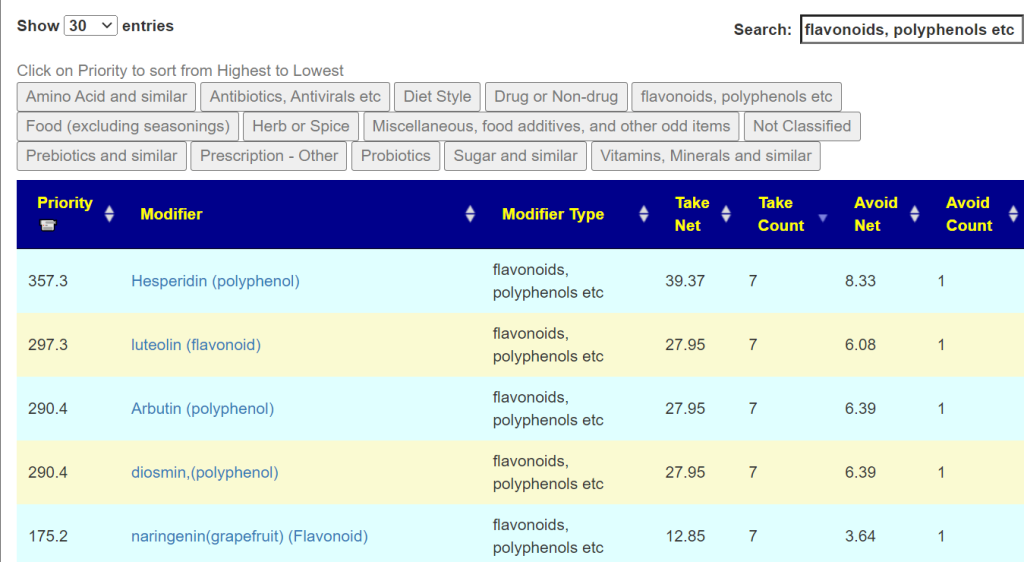
I would then go thru the list and cross out items that are not shown with at least 7 of the possible 8 in the technical details.
Bottom Line
My own experience with recovery was that it took about a year for many symptoms to wear off. The body is not an electronic device with an on/off switch; think of a meadow that has been damaged by fire, flood, or chemical spill — it takes time for things to come back.
Postscript – and Reminder
I am not a licensed medical professional and there are strict laws where I live about “appearing to practice medicine”. I am safe when it is “academic models” and I keep to the language of science, especially statistics. I am not safe when the explanations have possible overtones of advising a patient instead of presenting data to be evaluated by a medical professional before implementing.
I can compute items to take, those computations do not provide solid information on rotations, dosages, etc.
I cannot tell people what they should take or not take. I can inform people items that have better odds of improving their microbiome as a results on numeric calculations. I am a trained experienced statistician with appropriate degrees and professional memberships. All suggestions should be reviewed by your medical professional before starting. Some suggestions may be counterindicated for other medications you are taking and medical conditions.
The answers above describe my logic and thinking and is not intended to give advice to this person or any one. Always review with your knowledgeable medical professional.